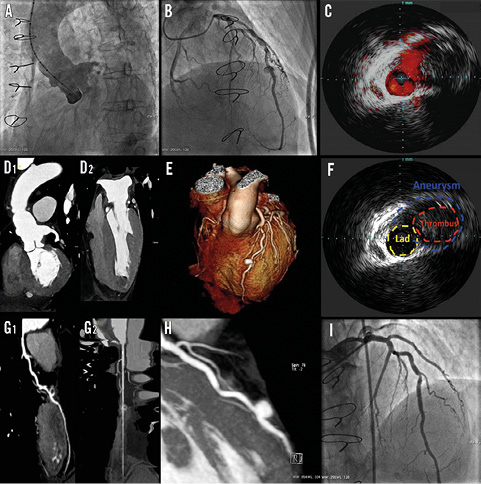
A 54-year-old male patient was admitted for non-ST-elevation acute coronary syndrome (NSTE-ACS). His medical history revealed previous normal coronary angiography, David’s valve-sparing surgery performed one year ago, and a diagnosis of a TGFBR2-associated Loeys-Dietz syndrome. Emergency catheterisation showed evidence of a normal ascending aorta with an ostial aneurysm of 15 mm of the re-implanted LCA, a saccular pouching of the middle LAD and a non-occlusive luminal thrombus of the apical segment of the LAD with a TIMI grade 3 flow (Panel A, Panel B). IVUS showed diffused intimal thickness of the LAD with a vessel dilatation of 7×10 mm and features highly suggestive of an aneurysm, partially obliterated by a round-shaped thrombus (Panel C, Panel F). A cardiac CT scan highlighted an apical ventricular thrombus, already suspected on echocardiogram, and the presence of a true aneurysm with an area of soft tissue density consistent with a thrombus of 6 mm (Panel D, Panel E, Panel G, Panel H). The coronary aneurysm was deemed suitable to be sealed with a 3.5×16 mm PTFE-covered stent (Panel I), and IVUS confirmed the complete apposition of the covered stent and exclusion of the aneurysm with no residual filling. The postoperative course was uneventful and the patient was discharged on DAPT plus warfarin. Management of an ACS due to an embolic coronary aneurysm in the context of an overlapping syndromic frailty of vessels and atherosclerotic process is challenging. A multidisciplinary clinical and imaging approach is essential to provide successful treatment (Moving image 1-Moving image 10).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Aortography.
Moving image 2. Angiography 1.
Moving image 3. Angiography 2.
Moving image 4. Angiography 3.
Moving image 5. Cardiac CT aneurysm.
Moving image 6. IVUS 1.
Moving image 7. IVUS 2.
Moving image 8. Angiography post-PTFE stent 1.
Moving image 9. Angiography post-PTFE stent 2.
Moving image 10. Angiography post-PTFE stent 3.
Supplementary data
To read the full content of this article, please download the PDF.
Aortography.
Angiography post-PTFE stent 3.
Angiography 1.
Angiography 2.
Angiography 3.
Cardiac CT aneurysm.
IVUS 1.
IVUS 2.
Angiography post-PTFE stent 1.
Angiography post-PTFE stent 2.