A 61-year-old man (height 181 cm, weight 110 kg) presented to our clinic with dyspnoea (NYHA Class II) and progressive chest and abdominal pain. Medical history included an aortic dissection type B with perfusion of the left kidney from the false lumen, diagnosed in 2009 (Figure 1A and Figure 1B). The patient was receiving five antihypertensive drugs (bisoprolol 5 mg ½-0-½, hydrochlorothiazide 25 mg 1-0-0, amlodipine 10 mg 1-0-0, urapidil 90 mg 1-0-1, moxonidine 0.3 mg 1-0-1). Office blood pressure (BP) was 160/95 mmHg. Ambulatory 24-hour BP monitoring confirmed true treatment resistance (mean 141/91 mmHg, non-dipping pattern).
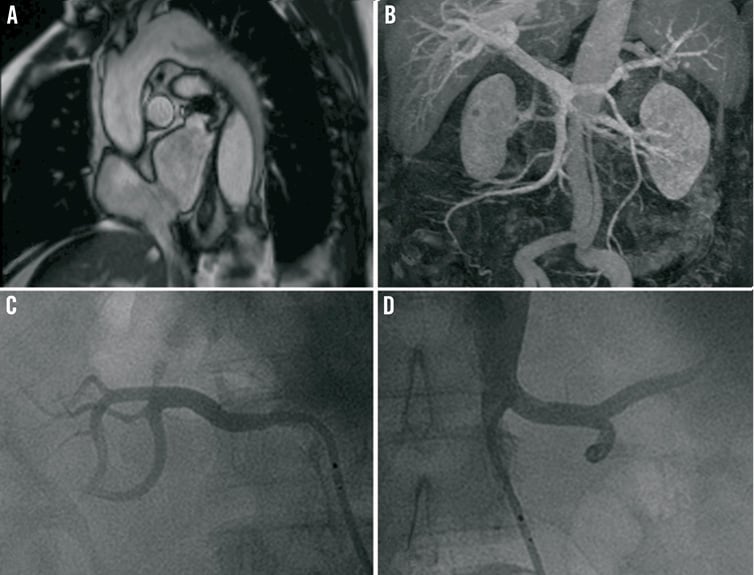
Figure 1. A) Magnetic resonance angiography (MRA) of the aortic arch, showing the entry of the dissection distal of the left subclavian artery. B) MRA, showing the descending aorta with the dissection membrane. Angiography of C) the right renal artery, and D) the left renal artery, before renal denervation (after fenestration).
Renal denervation was performed via femoral access. An 8 Fr IMA guiding catheter (Cordis, Johnson & Johnson, Warren, NJ, USA) was placed into the true aortic lumen at the level of the left renal artery. After a fenestration manoeuvre of the intima flap, performed using an IRON MAN PTCA wire (Abbott Vascular, Redwood City, CA, USA), the Symplicity™ radiofrequency catheter (Medtronic Inc., Minneapolis, MN, USA) was introduced and advanced to the distal segment of the renal artery under fluoroscopy (Figure 1C and Figure 1D, Moving image 1 and Moving image 2). Five treatments of the left artery and six of the right artery were successfully applied.
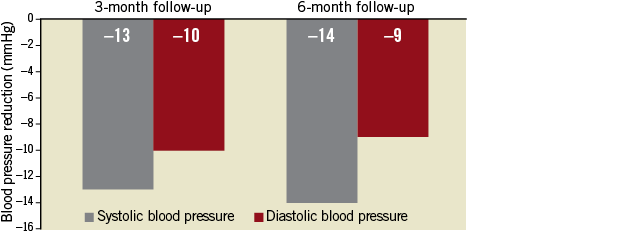
At three and six-month follow-up, ambulatory 24-hour BP was reduced by 13/10 mmHg and 14/9 mmHg (mean daytime 130/83 mmHg; mean night-time 122/79 mmHg), respectively (Online Figure 1). Six months after treatment, BP was controlled to target (office 130/90 mmHg). MRA showed no sign of complications at six-month follow-up.
Conflict of interest statement
The institution has received scientific support from Medtronic/Ardian. M. Böhm and F. Mahfoud have received speaker honoraria and consultancy fees from Medtronic/Ardian and are supported by Deutsche Forschungsgemeinschaft (KFO 196). F. Mahfoud is supported by Deutsche Hochdruckliga. S. Ewen has no conflicts of interest to declare.
Online data supplement
Online Figure 1. Blood pressure reduction after renal denervation in a patient with aortic dissection type B after three and six months (ambulatory 24-hour blood pressure monitoring).
Moving image 1. Angiography of the right renal artery, before renal denervation (after fenestration).
Moving image 2. Angiography of the left renal artery, before renal denervation (after fenestration).
Online Figure 1. Blood pressure reduction after renal denervation in a patient with aortic dissection type B after three and six months (ambulatory 24-hour blood pressure monitoring).
Supplementary data
To read the full content of this article, please download the PDF.
