Introduction
Functional tricuspid regurgitation (FTR) is the most frequent aetiology of tricuspid valve (TV) pathologies and is associated with increased morbidity and mortality1. Assessment and management of FTR has developed substantially, in particular because of the increased understanding of the long-term consequences of TV disease together with continued advances in transcatheter techniques2. Catheter-based repair requires detailed knowledge of the anatomy of the TV apparatus for planning and periprocedural assistance3. Particularly important is the right coronary artery (RCA), which is separated from the tricuspid annulus (TA) by only a few millimetres4.
This study comprehensively assessed the dynamic anatomic relationship between the TA and RCA in normal subjects and in patients with severe FTR.
Methods
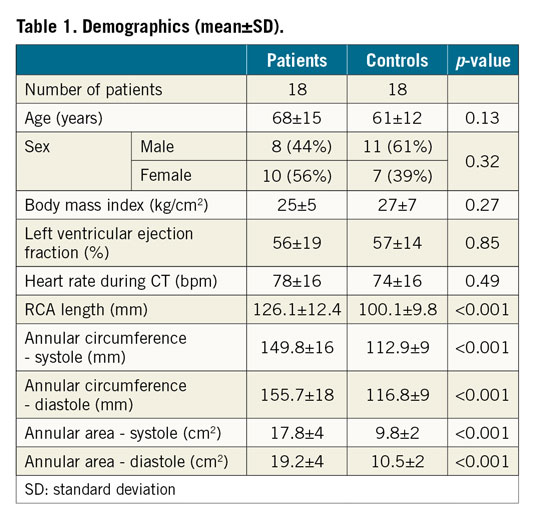
Eighteen patients with severe FTR, determined by transthoracic echocardiography, termed “patients”, and 18 patients without cardiac disease, termed “controls”, undergoing computed tomography (CT) were included (Table 1). All subjects had right dominant coronary supply.
CT DATA ANALYSIS
Image analysis was carried out using a prototype advanced visualisation, segmentation and image analysis software (3mensio Structural Heart 6.0 beta; Pie Medical Imaging, Maastricht, the Netherlands). TA and RCA dimensions, and distances between the TA and RCA were measured in all phases by two independent readers.
Details regarding CT protocol and statistical analysis can be found in Supplementary Appendix 1 and Supplementary Appendix 2.
Results
DIMENSIONS AND GEOMETRY OF THE TA AND RCA
Patients had a flatter TA and a flatter course of the RCA, coursing in the same plane as the TA, as compared to controls (difference between three-dimensional [3D] and two-dimensional [2D]: maximum lateral diameter in patients: 1.3 mm; in controls 1.5 mm) (Figure 1).
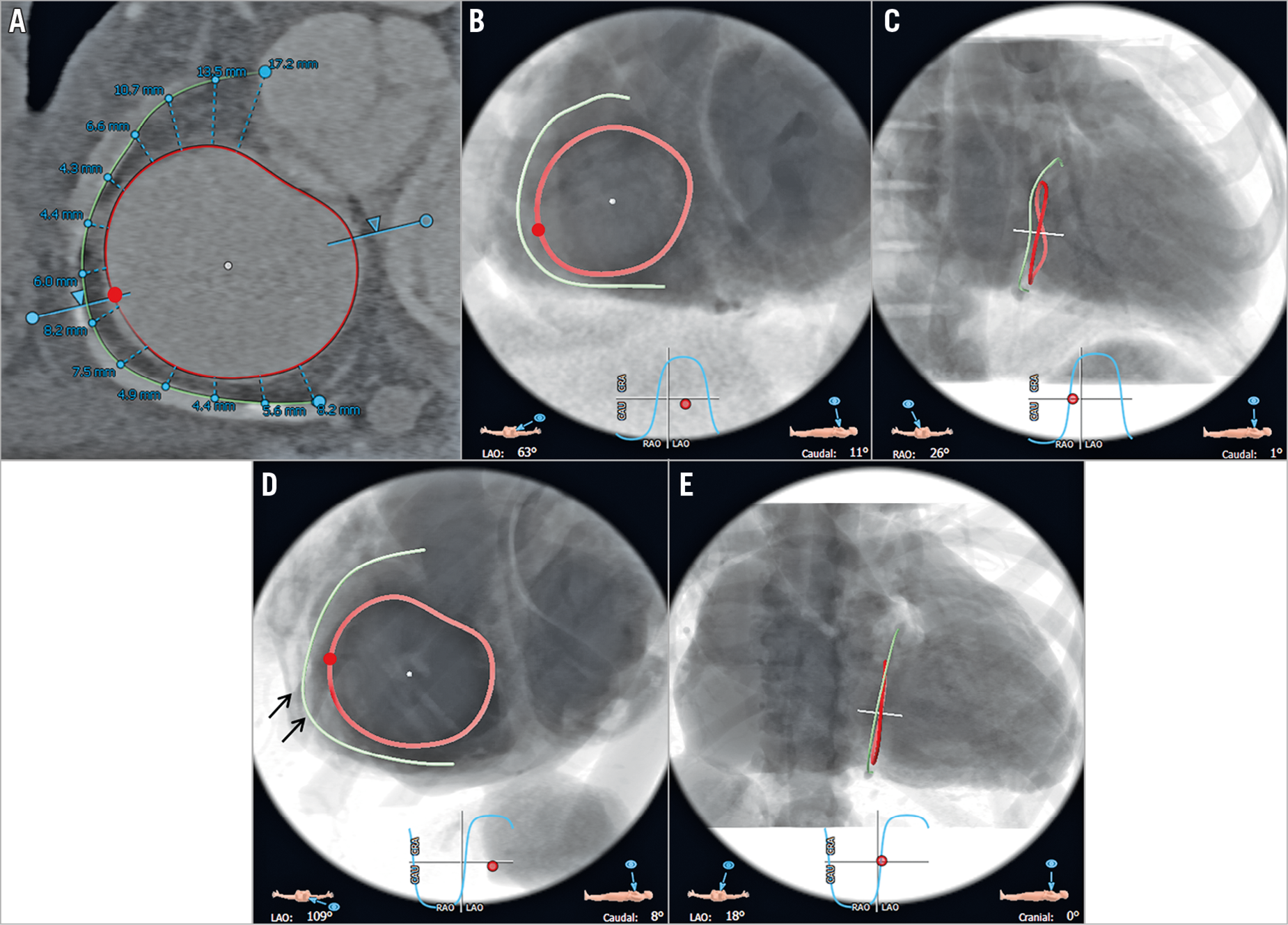
Figure 1. CT and fluoroscopic views of the TA and RCA in a control and a patient in diastole. CT (A) and fluoroscopic views of the TA and RCA in a control (B: 63° LAO; C: 26° RAO) and a patient (D: 109° LAO; E: 18° LAO) in diastole (80%), including distance measurements of 13 seed points in this representative patient (average number of seed points n=10). Red points: APC (B & D). Black arrows: short segment of the mid RCA in patients with consistent increase in distance to the TA (D), opposite the APC.
TA areas and circumferences were significantly larger and the RCA was significantly longer in patients than in controls in all phases (p<0.001) (Table 1, Supplementary Table 1).
Distances between the TA and RCA were significantly larger in patients than in controls for all measurement points and all phases (p=0.002-0.005) (Figure 2). In controls, the distance between the TA and RCA continuously decreased from proximally to distally throughout phases, while patients had a short segment with increasing distances (seed points 8/9) (Figure 1, Table 2). Both groups showed significantly larger distances proximally than distally (p=0.005-0.01).
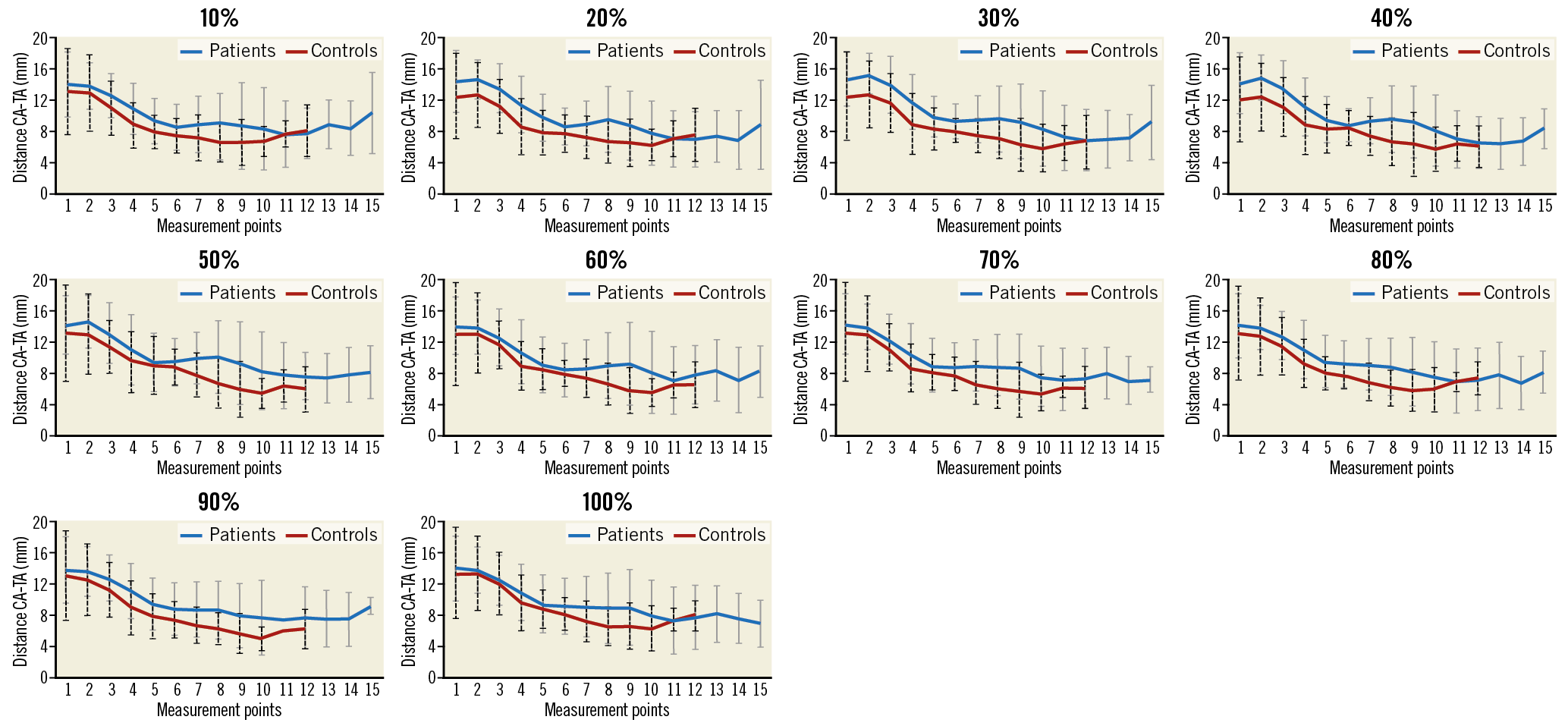
Figure 2. Distances and SD between the TA and RCA for all measurements and phases in patients (blue line; SD: grey fat line) and controls (red line; SD: black dashed line).
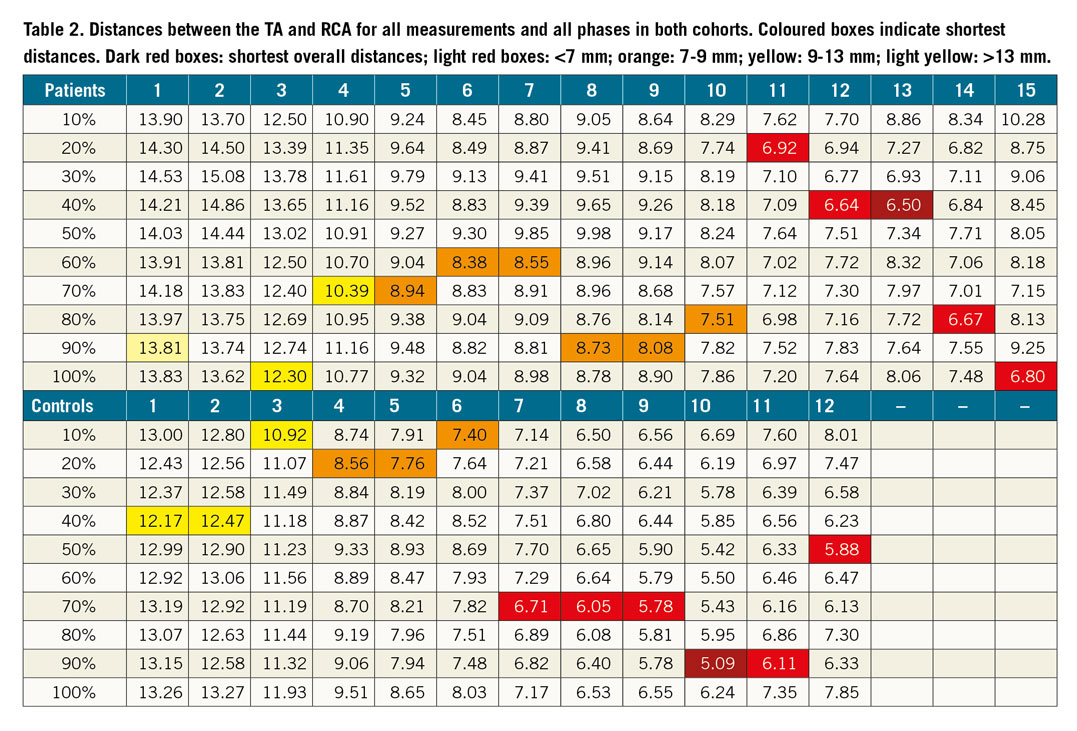
The shortest distance between the TA and RCA was found in patients in the distal RCA in end-systole (40%), while in controls the shortest distance was in the distal RCA in end-diastole (90%) (Table 2).
Movement of the RCA in relation to the TA throughout phases, measured between mid-systole (30%) and mid-diastole (70%) showed the largest displacement between the RCA and TA in the mid RCA in controls, while proximal and distal RCA segments showed less movement. Patients showed the largest displacement in proximal and distal segments and less motion in the mid RCA (Supplementary Figure 1).
Discussion
We found consistently longer distances between the TA and RCA in patients compared to controls. Distances between the TA and RCA showed a progressive decrease in both groups, being significantly larger proximally than distally, probably due to the larger distances of the proximal/ostial epicardial RCA compared to distal intramuscular segments. Our analyses confirm previous results4 showing the shortest distances between the posterior TA and distal RCA segment in patients with values between 5.1 and 5.5 mm.
In patients, but not in controls, we consistently found a short segment in the mid-distal RCA, opposite the anteroposterior commissure (APC), showing increasing distance to the TA. This could be explained by differences in the motion patterns of the TA with lower contraction in the anteroseptal to posterolateral direction in patients than in controls, as reported with echocardiography by Fukuda et al5. This finding might be relevant as many transcatheter TV replacement techniques target the APC for placing devices.
Limitations
The retrospective design, the small number of patients (none with left coronary dominance), and the study not being performed for a specific device are all limitations.
Conclusion
Our study demonstrates detailed analyses of dynamic 3D motion between the TA and RCA in controls and in patients throughout phases. Distances were larger in controls and continuously decreased from proximally to distally except for a short segment in the mid to distal RCA opposite the APC, where larger distances were found in patients only. This is an important landmark for annuloplasty devices.
|
Impact on daily practice Transcatheter therapies for FTR require pre-interventional imaging of the TV geometry and its relationship to surrounding structures such as the RCA to avoid impingement and occlusion of the RCA. |
Conflict of interest statement
M. Taramasso is a consultant for St. Jude Medical, and also reports personal fees from Abbott Vascular, Boston Scientific, 4Tech, Edwards Lifesciences and CoreMedic, outside the submitted work. F. Maisano is a co-founder of 4Tech, a consultant for Abbott Vascular, St. Jude Medical, Medtronic and Valtech Cardio, receives royalties from Edwards Lifesciences, and also reports personal fees from Abbott, Edwards Lifesciences, Mitraltech, and other from Edwards Lifesciences, Mitraltech and 4Tech, outside the submitted work. The other authors have no conflicts of interest to declare.