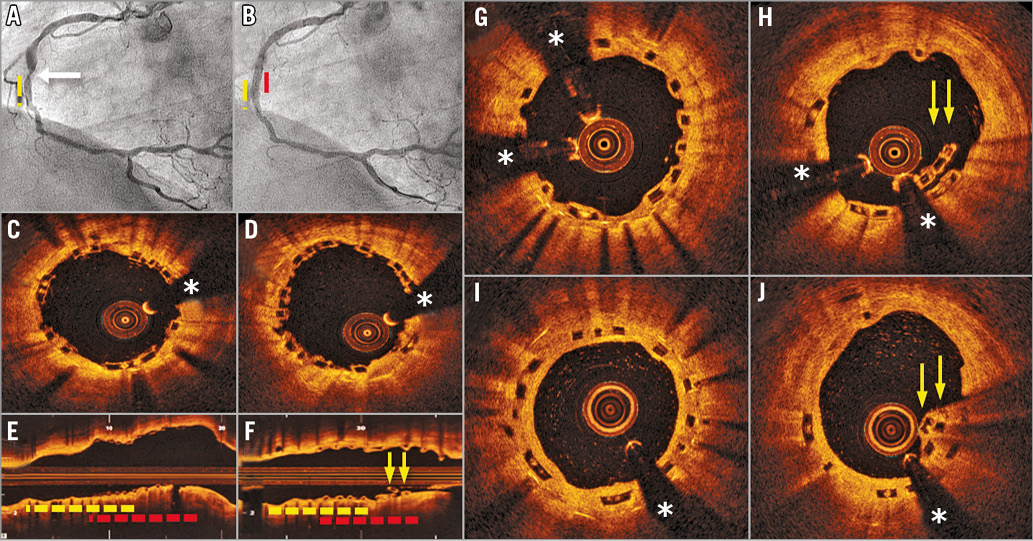
A 61-year-old woman presented with effort angina one year after the implantation of a drug-eluting stent (DES) in the mid right coronary artery (RCA). Coronary angiography revealed a proximal “edge” in-stent restenosis (Panel A, arrow; yellow broken line: DES) that was successfully treated with a 3×8 mm bioresorbable vascular scaffold (BVS) (Absorb™; Abbott Vascular, Santa Clara, CA, USA) at 20 bar (Panel B, red broken line: BVS). Optical coherence tomography (OCT) confirmed an excellent expansion and apposition of the BVS (Panel C-Panel E, yellow broken line: DES; red broken line: BVS). One month later she was admitted for an inferior acute myocardial infarction. Urgent coronary angiography showed a good result of the BVS but complete occlusion of the most distal RCA that was treated with a new DES. On OCT, the BVS was covered by incipient bright neointima. However, a localised malapposition of some BVS struts was readily identified leading to the diagnosis of late scaffold fracture (Panel F-Panel H, arrows). No further intervention was made. At eight-month follow-up, the BVS maintained an excellent angiographic result and OCT revealed complete neointimal coverage of the fractured BVS (Panel I, Panel J, arrows) (*denotes wire artefact).
Stent fracture is a rare complication described in metallic stents and, more recently, also in BVS. Stent fracture is associated with major complications including restenosis, aneurysm/pseudoaneurysm formation and thrombosis. Risk factors include high implantation pressures and hinge point location. Our BVS was implanted at high pressures but not at a hinge point. The fracture was detected well before the time required for resorption-induced structural BVS disintegrity. Iatrogenic mechanical disruption can never be completely discarded but no clues were identified in this regard. Notably, the BVS rupture was located precisely at the edge of the previous DES. The potential interaction of the rigid underlying DES platform with the flexible overlapping BVS structure should be investigated. To the best of our knowledge, this is the first description of a delayed fracture in a BVS implanted for in-stent restenosis.
Conflict of interest statement
The authors have no conflicts of interest to declare.