Coronary obstruction remains one of the most worrisome life-threatening complications of transcatheter aortic valve implantation (TAVI)1. While its incidence is low (<1%) in native aortic valves, it increases by ~4 to 6 times in the presence of a surgical aortic bioprosthesis (valve-in-valve [VIV] TAVI) (Figure 1)1,2. Current therapeutic approaches for such patients are still suboptimal (coronary wire/stent protection with bail-out snorkelling stenting and coronary artery bypass graft)1,3. The use of transcatheter electrosurgery for aortic leaflet laceration to prevent iatrogenic coronary artery obstruction (BASILICA) in TAVI procedures has emerged as a promising technique in this setting, but the experience remains very limited4.
In this issue of EuroIntervention, Kitamura and colleagues evaluated, in a single-centre experience, the feasibility, efficacy and safety of the BASILICA technique in TAVI patients at high risk of coronary obstruction5.
A total of 23 leaflets in 21 consecutive patients were included (90% and 10% degenerated bioprosthetic and native leaflets, respectively). BASILICA was feasible in all but one patient (95%) and resulted in effective prevention of coronary obstruction in 19 patients (90%). One patient developed a non-flow-limiting ostial lesion after BASILICA and TAVI, ultimately requiring left main coronary stenting. The complication rate was low, with no cases of major vascular complications, need for mechanical circulatory support, stroke or mortality at 30 days. However, up to 30% of the patients required vasopressor support following leaflet laceration. These results provide further evidence on the feasibility, efficacy and relative safety of the BASILICA technique in TAVI recipients at risk of coronary obstruction. Some aspects of Kitamura’s work and the BASILICA technique merit further discussion.
Safety
The BASILICA technique requires the use of various sheath accesses, frequent exchange of catheters, and calcified leaflet manipulation. This has been associated with relatively high rates of vascular complications, stroke, injury of non-target structures, and haemodynamic compromise due to severe aortic regurgitation after leaflet splitting4. Kitamura’s safety results compare favourably with those reported in prior studies, particularly regarding cerebrovascular events. The nearly systematic use of embolic protection devices in Kitamura’s series may have played a role, and should probably be considered in future studies. Despite these good safety results, the BASILICA technique remains technically challenging and potentially associated with life-threatening complications, which would support the implementation of this technique only at highly experienced centres and with surgical backup.
Efficacy
The BASILICA trial showed a high efficacy of the leaflet laceration technique in TAVR cases4. The results of Kitamura’s work further confirm these findings in a real-world setting. While it would be more difficult to evaluate the real risk reduction regarding coronary obstruction events, the 4.6% rate of coronary obstruction reported by Kitamura et al seems to be low given this very high-risk population, where a predicted incidence of probably >50% of partial or complete coronary obstruction would be expected (Figure 1). Interestingly, recent data suggested a mitigation of neosinus flow stasis following BASILICA, which may potentially reduce the risk of transcatheter valve leaflet thrombosis6. Of note, no cases of subclinical valve thrombosis were observed among the 15 patients who underwent multidetector computed tomography (MDCT) imaging at follow-up in Kitamura’s study. Finally, future studies will need to evaluate the potential efficacy of the BASILICA technique to facilitate coronary access, particularly considering the high rate of CoreValve®/Evolut™ systems (Medtronic, Minneapolis, MN, USA) used in VIV procedures7.
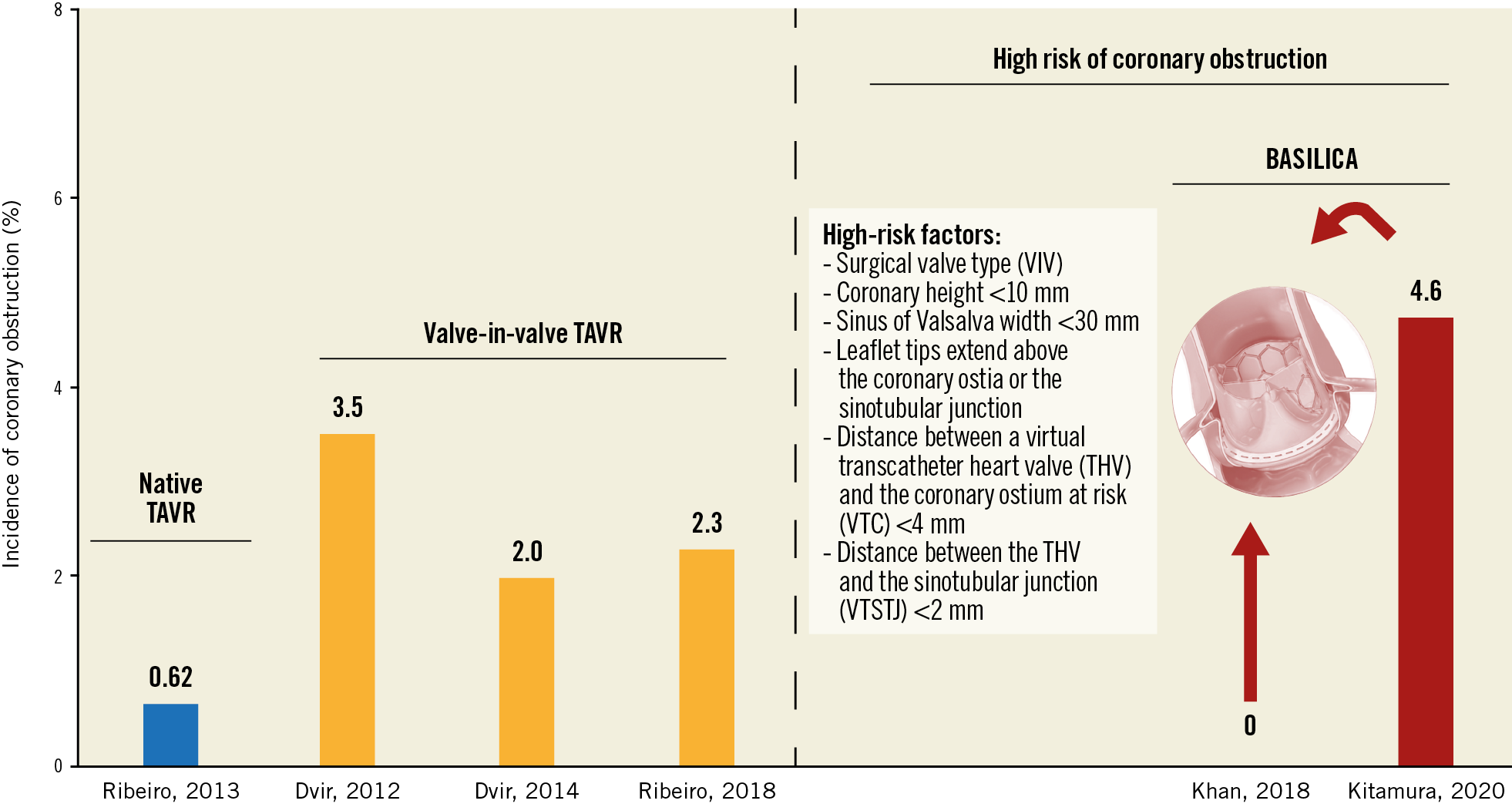
Figure 1. Incidence of coronary obstruction in the main studies in the context of native and valve-in-valve TAVR, as well as during TAVR in patients with high-risk features for this complication, including those undergoing the BASILICA technique1,2,4,5.
Patient selection
While increasing experience and technique refinements have translated into progressive improvements in the results of BASILICA, questions remain regarding the target population, where the risks of coronary obstruction would clearly exceed the risks associated with leaflet tearing. Coronary height <10 mm, sinus of Valsalva width <30 mm, leaflet tips extending above the coronary ostia or the sinotubular junction, the distance between a virtual transcatheter heart valve (THV) and the coronary ostium at risk (VTC) <4 mm, and/or at the sinotubular junction (VTSTJ) <2 mm have been identified as risk factors for coronary obstruction post TAVR1,2,4,5. However, in VIV cases, only VTC <4 mm and valve type (stented with externally mounted leaflets or stentless) but not coronary height were identified as predictors of coronary obstruction2. The vast majority of patients included in Kitamura’s series were VIV cases, but only about half of them had either a valve type or a VTC measurement indicating an increased risk. Unfortunately, the authors failed to specify whether all patients had at least one of these two factors. This aspect is of great importance, as the BASILICA technique remains a preventive treatment and can be associated with some important complications; overtreatment should therefore be avoided. In some patients, alternative techniques such as simultaneous coronary angiography or aortography during balloon inflation or partial deployment of a self-expanding valve (with the possibility of valve recapture) can be performed for further determination of the risk of coronary obstruction and the need for the BASILICA technique. Also, future studies using advanced MDCT imaging, possibly with virtual simulation, in addition to the potential yield of 3D modelling, are warranted.
In conclusion, transcatheter leaflet laceration has emerged as a preventive technique to avoid coronary obstruction during TAVI procedures. The study of Kitamura et al confirms the efficacy and safety of this technique in a real-world setting, and provides further support for its extended application at experienced centres. However, the lack of randomised data makes it difficult to estimate the real risk/benefit of these procedures, and highlights the need for larger studies with improved predictive models to define more clearly the specific risk of coronary obstruction for each individual patient along with an accurate evaluation of the different preventive techniques.
Conflict of interest statement
J. Rodés-Cabau has received institutional research grants from Edwards Lifesciences, Medtronic and Boston Scientific, and holds the Research Chair “Fondation Famille Jacques Larivière” for the Development of Structural Heart Disease Interventions. H. Ribeiro is a proctor for Boston Scientific, Medtronic and Edwards Lifesciences and has received a research grant from Medtronic.
Supplementary data
To read the full content of this article, please download the PDF.