During the last decade, extensive literature has confirmed the high diagnostic accuracy of coronary computed tomography angiography (CCTA) for the detection of coronary stenosis using invasive coronary angiography (ICA) as gold standard1. Based on these data and the findings of large prospective trials, such as PROMISE and SCOT-HEART, CCTA has been definitively integrated into the routine clinical management of patients with suspected coronary artery disease (CAD) as the first-line diagnostic and prognostic method2,3. The ESC Guidelines on the management of stable CAD recommend CCTA with a Class I level of evidence4. However, relying only on anatomical information with CCTA has proven to be insufficient to detect haemodynamically significant epicardial stenosis5. Recently, CT-derived fractional flow reserve (FFRCT) and stress myocardial CT perfusion (CTP) have emerged as technologies for a comprehensive evaluation of coronary stenosis, offering both anatomical (i.e., luminal and plaque) and functional assessment in one single technique. In particular, FFRCT is a well validated method for the non-invasive evaluation of coronary physiology with high agreement with invasive FFR6. Growing evidence supports ICA deferral when FFRCT is negative and a higher PCI/ICA ratio when decisions around ICA are FFRCT-guided7. However, the commercially available option for FFRCT computation still requires image data transfer to external supercomputers and remains time-consuming, whereas, for more rapid FFRCT derivation, simplified on-site workstation-based prototype algorithms have been developed with promising results8. In this issue of EuroIntervention, Westra et al report a prospective multicentre study aimed at assessing the diagnostic performance of a novel CCTA-based method for on-site calculation of FFR (CT-QFR) in 278 symptomatic patients9.
The diagnostic performance of CT-QFR was compared with myocardial perfusion scintigraphy (MPS) and cardiovascular magnetic resonance (CMR) as second-line tests (randomised 1:1) in patients presenting with obstructive CAD on CCTA, by using invasive FFR as standard of reference. Patient-level diagnostic accuracy was better for CT-QFR than for both MPS (82.2% vs 70.3%, p=0.029) and CMR (77.0% vs 65.5%, p=0.047). Following a positive CCTA and with the intention to diagnose, CT-QFR, CMR and MPS were equally suitable as rule-in and rule-out modalities, with better sensitivity of CT-QFR. A strength of the study which is worthy of mention is that the authors compared the CT-QFR results with those of two largely validated stress tests, namely CMR and MPS, both recommended in the Guidelines (level of evidence 1)4, demonstrating CT-QFR to be a promising tool to detect flow-limiting stenosis. As a potential weakness of the method, the rate of unfeasible CT-QFR was not negligible (17% of CCTAs). Regarding the alternative functional CT-based method, stress CTP requires an additional scan, use of a stressor agent and is associated with higher radiation exposure but, on the other hand, may provide information on both macrovascular and microvascular disease status10 (Figure 1). In summary, functional assessment with CTP or FFRCT can improve decision making in patients with CAD detected at CCTA.
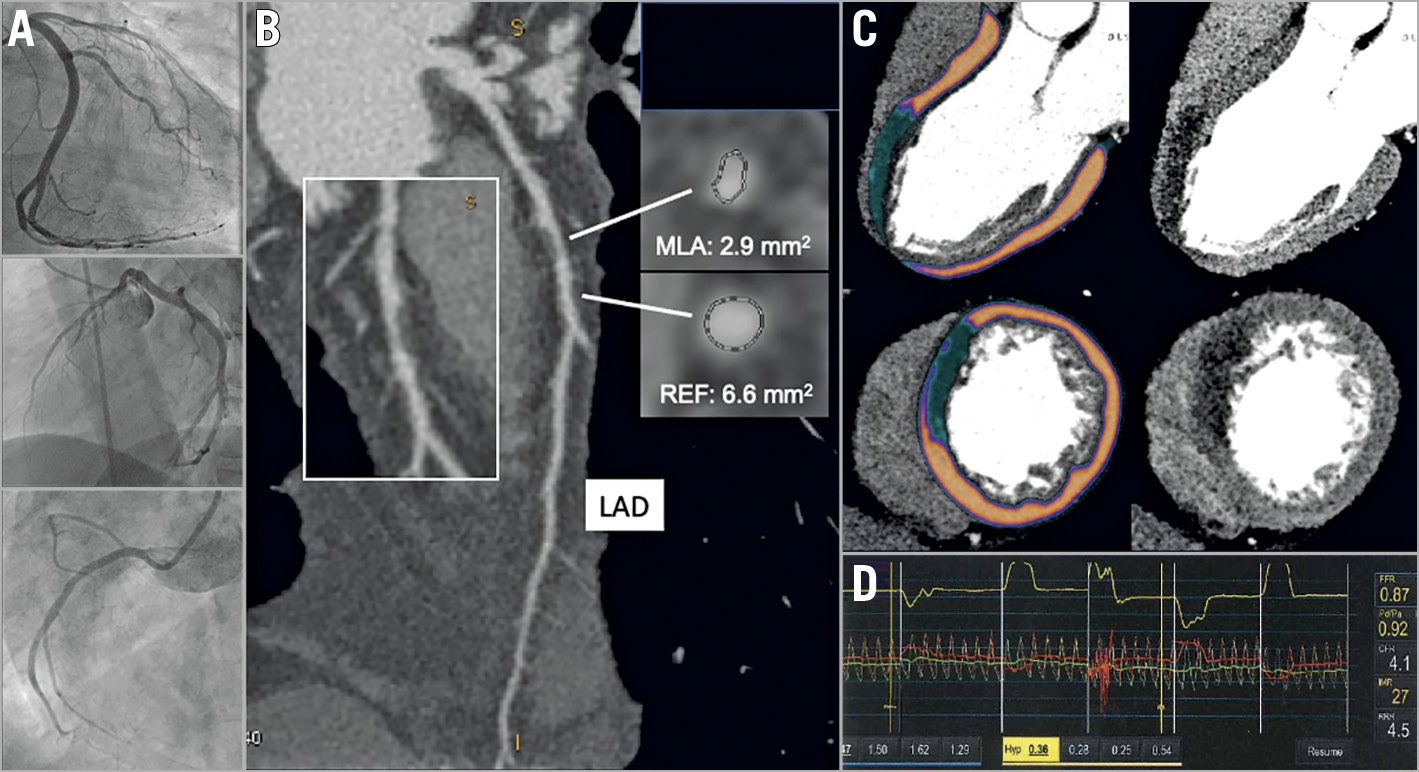
Figure 1. Myocardial ischaemia detected by stress CT perfusion. A 54-year-old man, previous PCI and DES in the mid-distal portion of a dominant left circumflex artery, symptomatic for exertional angina. ICA was negative for in-stent restenosis or de novo stenosis (A). CCTA showed an intermediate stenosis (50-55%) in the middle portion of the left anterior descending artery (LAD), with a minimal lumen area of 2.9 mm2 at cross-sectional reconstruction (B). Stress CTP long- and short-axis reconstructions (C) showed a transmural perfusion defect of the anterior interventricular septum. Invasive physiological assessment (D) demonstrated microvascular dysfunction in the territory of the LAD without functional relevance of the epicardial stenosis (IMR=27, FFR=0.87).
Conflict of interest statement
The author has no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.