![]()
Abstract
In a ranking of the gross domestic product per capita in 2015, Belgium ranked 19th in the world according to the International Monetary Fund and the World Bank. It has a Human Development Index of 0.890, in which it is preceded by only 20 other countries in the world. This is, at least in part, due to a well-developed social security system on which all citizens can rely. Over the last 5-10 years, however, this system has come under increasing pressure. This has resulted in insufficient, incomplete and late reimbursement of all technologies that were introduced over the last ten years in the cathlab: intracoronary imaging techniques are not reimbursed at all, and FFR only to a vastly insufficient degree. For several structural heart interventions, a system of limited and incomplete reimbursement has recently been set up, with a requirement to organise these procedures within the frames of hospital networks.
Numbers of PCIs have risen by 15% over the last four years, coinciding with an increase in the number of cathlabs by 50%, aiming at better access to primary PCI for STEMI patients. This has also resulted in a decrease in the average procedure volume per centre. Two thirds of PCIs are performed via the radial access. DES penetration has increased to 74%, approaching 100% in some centres, while the uptake of BRS has been very limited so far.
Demographics and organisation
For a population of 11.4 million people, Belgium counts 49 cathlabs which all provide a 24h/7d service, as required by law. Of these hospitals, thirty have on-site cardiac surgery. As no official certification in interventional cardiology exists, the exact number of operators is unknown. In 2015, 219 cardiologists performed at least one percutaneous coronary intervention (PCI), with a very wide range in annual numbers of procedures per operator.
The Belgian Working Group of Interventional Cardiology (BWGIC) has maintained an online registry on coronary interventions for over 12 years, to which all cathlabs report their coronary procedures. In 2012, however, this registry moved to the national authorities, as a requirement for reimbursement of materials. In recent years, national registries, organised by the BWGIC, have been set up regarding transcatheter aortic valve implantation (TAVI), MitraClip® (Abbott Vascular, Santa Clara, CA, USA) and left atrial appendage (LAA) closure. Due to inadequate funding, audits are minimal.
To optimise communication with its members (all interventional cardiologists in Belgium), the BWGIC has set up a website (www.bscardio.be/working-groups/belgian-working-group-oninterventio nal-cardiology-bwgic/).
Reimbursement for coronary interventions consists of an honorary fee and a fixed lump sum for all materials used during the procedure. The latter is higher in case of multivessel PCI. There is no reimbursement for any of the intracoronary imaging techniques, and flow/pressure techniques are refunded to a vastly insufficient degree. Only recently has some reimbursement been introduced for TAVI, limited to 500 cases/year for the whole country, and MitraClip (140 cases/year, increasing to 200/year over the next four years). This regulation on valve interventions requires hospitals to form networks to plan and perform these procedures together. Funding for LAA closure has been in effect since the beginning of 2017.
As Belgium has a system of compulsory social security, all citizens have reimbursement for the major part of all interventions.
The BWGIC is in the process of negotiating with the authorities the terms and conditions of a certification in interventional cardiology.
Coronary interventions
Since 2012 the annual number of coronary angiographies has increased by 3%, while the number of PCIs has grown by 15% (Table 1). This coincides with the opening of 16 new cathlabs over the last four years, and each cathlab is required to reach a minimum of 300 PCIs per year. As almost all ST-elevation myocardial infarctions are treated by means of primary PCI, the number of primary PCIs has risen by almost 20% over the last three years. PCI for restenosis comprises 7% of the total volume. As a result of the higher number of cathlabs, the average PCI volume per cathlab has decreased to 551 cases per year. Remarkably, the average number of procedures per operator has remained constant, albeit with a very wide range, as stated above. PCIs without implantation of a stent represent about 5% of all procedures. The proportion of drug-eluting stents (DES) has increased from 63% to 74% between 2013 and 2015, and is virtually 100% in some centres. The uptake of bioresorbable scaffolds (BRS) has been very slow in Belgium, with only 467 BRS implanted in 2015. This is, at least in part, due to the fact that these devices are more expensive as such, with a higher usage of balloons for predilatation and post-dilatation, while reimbursement is identical to that for a regular DES.
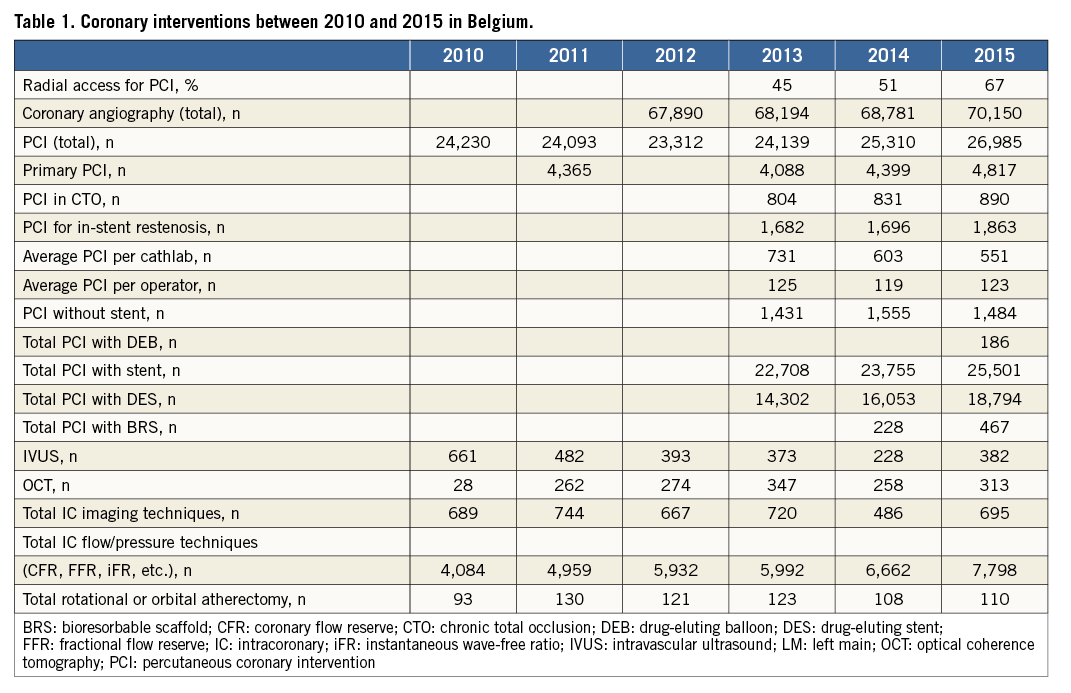
Regarding intracoronary imaging techniques, annual numbers have remained stable over the last six years, with optical coherence tomography (OCT) increasingly replacing intravascular ultrasound (IVUS), up to 45% in 2015. The relatively low use of these techniques as compared to the total number of PCIs is explained entirely by the lack of any specific reimbursement for intracoronary imaging. A substantial proportion of these techniques is used in the setting of clinical trials.
While reimbursement for fractional flow reserve (FFR) measurements covers less than half of the actual costs, the number of FFR wires used has almost doubled between 2010 and 2015, from 4,084 to 7,798.
Rotational atherectomy is used in less than 0.5% of all PCIs, and this proportion has remained stable over the last six years.
Structural heart interventions
Despite the lack of any reimbursement until very recently, more than 300 TAVIs were performed per year between 2010 and 2014, and 465 in 2015 (Table 2). As stated above, a partial reimbursement for 500 TAVIs per year has recently been introduced, which will undoubtedly lead to a further rise in this number, but most probably not above 700 annually. Approximately 83% of all TAVIs are performed via the transfemoral route.
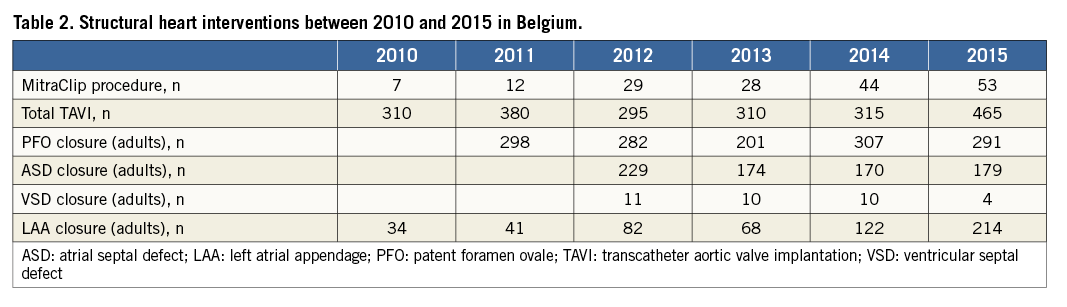
The number of MitraClip procedures has slowly grown, up to 53 in 2015. In view of the new reimbursement regulation, this number is expected to grow to 200/year over the next four years. Within this regulation, these procedures are concentrated within seven hospital networks nationwide.
The numbers of closures of patent foramen ovale and atrial septal defect have remained stable over the years, at around 290 and 180 per year, respectively. Ventricular septal defect closures remain rare interventions.
Transcatheter left atrial appendage occlusion (LAAO) started in Belgium in 2009 and has increased over time, up to more than 200 implants per year. Since 2011, data on all procedures are collected in a national registry by 13 participating centres. Reimbursement for LAAO has been available since the beginning of 2017.
Limitations
The numbers in this paper have been collected via different methods: coronary procedures before 2012 and structural procedures (TAVI, MitraClip and LAA closure) were collected through an electronic questionnaire, organised by the Belgian Working Group of Interventional Cardiology, on a voluntary basis with little or no audit of source data. Hence, while we believe that these figures are trustworthy, we cannot be absolutely certain. The data corresponding to the coronary procedures after 2012 were collected by the national authorities as a requirement for reimbursement of materials, which ensures the solidity of the numbers of PCIs. As there is no systematic audit of other aspects of these procedures, e.g., the use of FFR and OCT, these numbers need to be interpreted with some caution.
Conflict of interest statement
All authors have no conflicts of interest to declare.
