A 73-year-old woman presented with severe mitral regurgitation and New York Heart Association (NYHA) Class IV symptoms. The patient was discussed in our Heart Team and deemed inoperable due to frailty and high surgical risk (Society of Thoracic Surgeons [STS] score: 15.1%). Transoesophageal echocardiography (TOE) showed severe mitral valve regurgitation with a diminutive posterior mitral valve leaflet and consecutive restricted leaflet motion (Moving image 1). An edge-to-edge repair was therefore not considered, but analysis of a full cardiac cycle by computed tomography depicted suitability for Tendyne (Abbott) implantation. Computational modelling revealed a high risk of left ventricular outflow tract obstruction (LVOTO) due to the excessive length (2.8 cm) of the anterior mitral valve leaflet (AML) and small LVOT dimensions (Figure 1A, Moving image 2). In the past, patients with a very tethered, floppy or long AML have been deemed unsuitable for Tendyne implantation: the covered prosthesis holds the native leaflets open during the whole cardiac cycle, and during early systolic outflow, the aforementioned, high-risk AML features can contribute to a “parachute configuration” of the native leaflet with a risk of LVOTO. To reduce the risk of systolic anterior movement post-implantation, AML modification is required.
A fairly new transapical, TOE-guided approach for AML laceration was considered, which has only been reported in one other clinical case1. The here presented case, however, offers pathophysiological insights as to why AML modification is necessary even for the implantation of a covered prosthesis like the Tendyne, and we provide the short-term clinical and echocardiographic follow-up.
After gaining transapical access, which is the standard access route for Tendyne, a surgical endoscopic scissor (CLICKLine; Karl-Storz) was inserted (Figure 1B, Moving image 3, Moving image 4) and positioned via a 26 Fr DrySeal sheath (W.L. Gore & Associates) into the left atrium, directly above the mitral valve annular plane. The stepwise pulling back of the sheath resulted in the insertion of the AML into the endoscopic scissor. After an echo-guided confirmation of the correct scissor position, directly underneath the anterior leaflet, successful cutting of the AML was achieved (Figure 1C) resulting in higher-grade mitral valve regurgitation (Moving image 5). Afterwards, a 29L LP Tendyne valve was successfully implanted (Figure 1D) without any complications. The final perioperative imaging assessment showed good anchoring of the valve with no leakage and a mean gradient of 4 mmHg. At 30 days, the patient presented with a substantially improved functional capacity (NYHA II), excellent prosthesis valve function and no relevant LVOTO (gradient 9 mmHg).
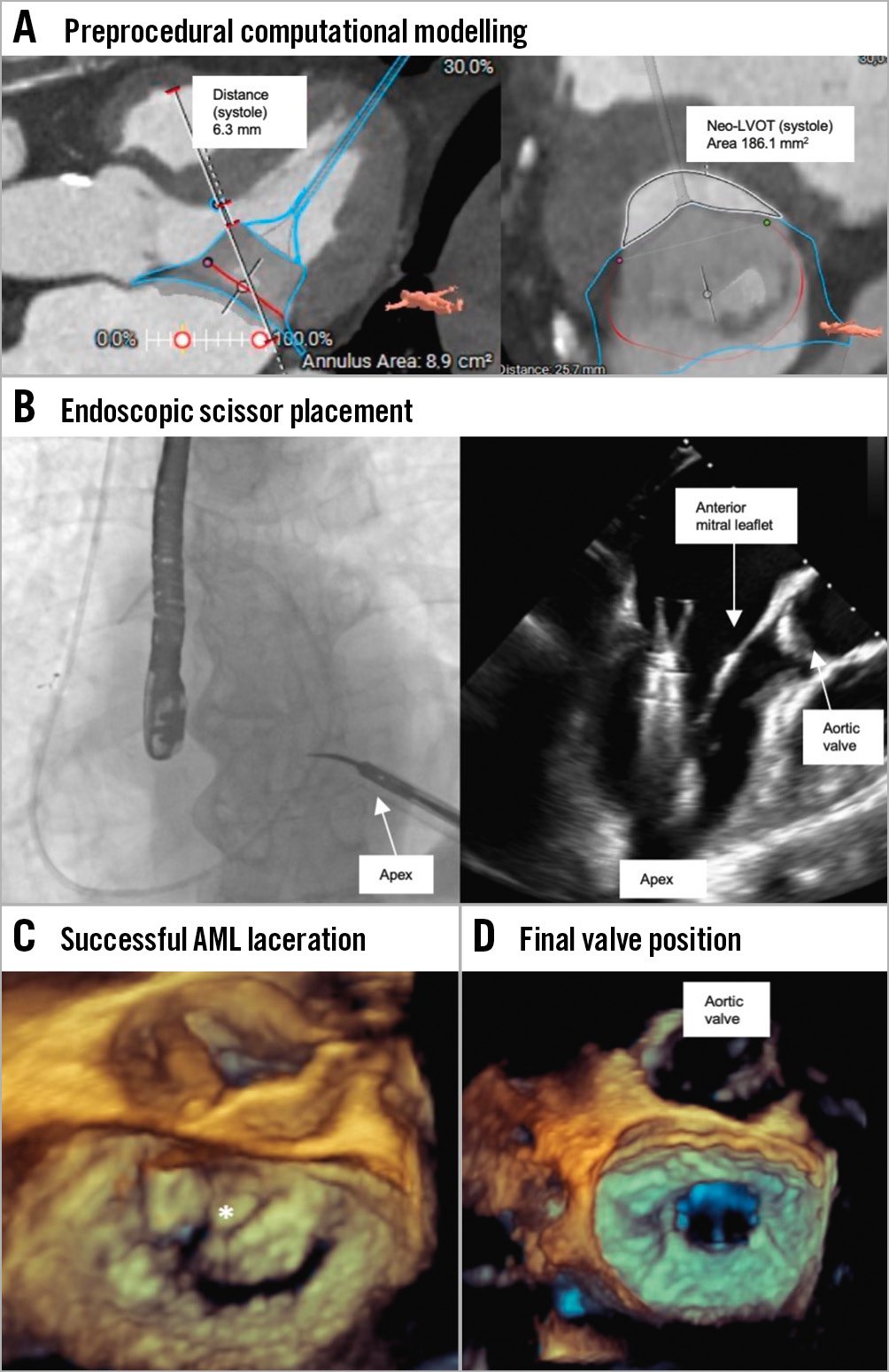
Figure 1. Anterior mitral leaflet modification with endoscopic scissors during Tendyne implantation. A) Computed tomography modelling of the Tendyne (Abbott) prosthesis with 3mensio (Pie Medical) revealed the predicted small neo-LVOT dimensions (area of 181.1 mm2) complicated by high-risk AML features favouring systolic anterior movement of the native leaflet post-implant. B) Fluoroscopic view of scissor insertion (left) and scissor placement (TOE LVOT view, right). C) Laceration of the anterior mitral leaflet (white asterisk). D) 3D-TOE view after final valve deployment. 3D: three-dimensional; AML: anterior mitral valve leaflet; LVOT: left ventricular outflow tract; TOE: transoesophageal echocardiography
Conflict of interest statement
A. Boening has received speaker honoraria from Abbott and is a co-founder of the Mitralklappen D/EU gGmbH. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. 3D-TOE surgical view of the mitral valve depicting a diminutive posterior mitral valve leaflet and consecutive restricted leaflet motion.
Moving image 2. Computational modelling of the Tendyne prosthesis position.
Moving image 3. 2D-TOE X-plane view of endoscopic scissor advancement from the apex.
Moving image 4. 3D-TOE reconstruction of the endoscopic scissor advancement (surgical view).
Moving image 5. 3D-TOE surgical view of the mitral valve showing high-grade mitral valve regurgitation after anterior mitral valve leaflet modification with endoscopic scissors.