Abstract
Aims: Snaring has recently been reported as being effective in catching the retrograde guidewire (GW) in retrograde percutaneous coronary intervention (PCI) for chronic total occlusion. However, commercially available snares and previously reported homemade snares have a number of drawbacks, such as additional cost, limited size adjustability, risk of vessel injury and difficult handling. We report here a novel method to create easily an inexpensive, safe and size-adjustable snare.
Methods and results: Our newly developed homemade snare consists of a conventional 0.014” GW, a PCI balloon, and a guiding catheter (GC). In most cases, no extra cost is needed. As the snare is created by the soft wire tip, vascular injury is negligible. To adjust the size of the snare loop, the snare wire is simply pulled backwards and pushed forwards. Using this snare technique, we succeeded in the total revascularisation of a CTO in the left main trunk with a retrograde approach.
Conclusions: We report a novel method to create easily an inexpensive, safe and size-adjustable snare, and demonstrate its use in a retrograde CTO intervention. In some cases where a conventional snare is indicated, such as removal of intravascular iatrogenic foreign bodies, this novel homemade snare would be preferable because of its advantages.
Description
We report here a novel method to create easily an inexpensive, safe and size-adjustable snare using a conventional 0.014” guidewire (GW), a percutaneous coronary intervention (PCI) balloon, and a guiding catheter (GC). In the setting of retrograde PCI for chronic total occlusion (CTO), the homemade snare can be helpful to catch the retrograde wire tip within the aorta.
History
Snaring is generally known to be an effective and minimally invasive technique to retrieve intravascular iatrogenic foreign bodies1. In addition, it has recently been reported as being effective in catching the retrograde GW in retrograde PCI for CTO2-4. However, commercially available snares and previously reported homemade snares have a number of drawbacks, such as additional cost, limited size adjustability, risk of vessel injury and difficult handling5.
Technical specifications
SET-UP AND USE OF OUR HOMEMADE SNARE
A conventional 0.014” GW is inserted into the wire lumen of a common PCI balloon and advanced until it protrudes 20 to 30 mm from the balloon tip (Figure 1A). The GW tip is folded back towards the balloon and the system (en bloc) is inserted into a GC through a Y-connector (Figure 1B). The PCI balloon and folded GW are positioned in the distal GC, around 20-30 mm from the tip (Figure 2A). After trapping the tip of the folded GW by balloon inflation (usually 8-12 atm) (Figure 2B), advancement of the GW shaft will produce a size-adjustable snare loop (Figure 2C, Figure 2D). The retrograde GW is advanced into the snare loop (Figure 3A) and caught by pulling back the GW of the homemade snare system (Figure 3B - Figure 3D). Once the retrograde GW is successfully pulled into the GC it can easily be released by deflating the balloon and pulling back the snare wire. Regular wire externalisation can now be performed as previously described6.
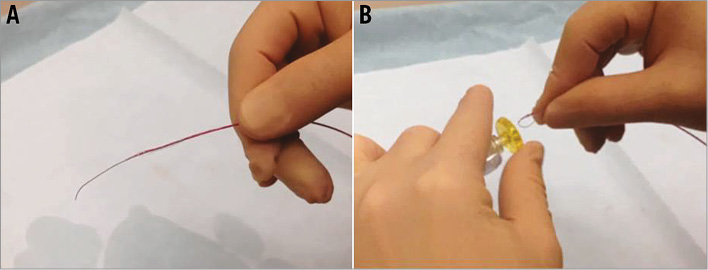
Figure 1. System preparation. The balloon is mounted on a soft guidewire (GW) and placed 20-30 mm from the tip of the GW (A). The GW tip protruding from the balloon tip is folded backwards and inserted into the Y-connector (B).
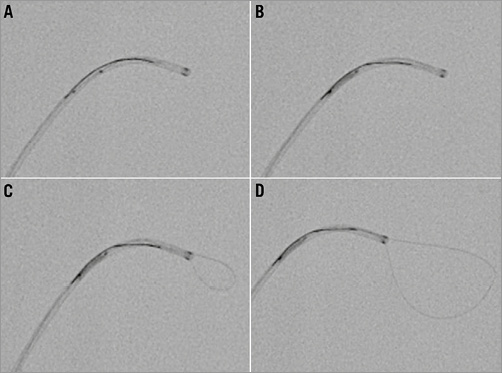
Figure 2. Creating a snare loop. The homemade snare system is advanced up to 20-30 mm from the tip of the guiding catheter (GC) (A). The balloon is inflated with enough pressure (8-12 atm) to trap the GW tip in the GC (B). As the GW of the homemade snare system is advanced, the snare loop will unfold from the GC tip (C). The size of the snare loop is adjusted by pushing and pulling the GW (D).
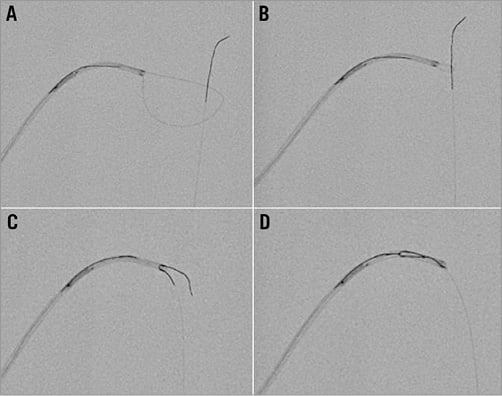
Figure 3. Catching a guidewire. The retrograde GW is advanced into the snare loop (A). By pulling back the snare GW (B), the tip of the retrograde GW is caught (C) and retrieved into the GC (D).
Indications for use
To catch the retrograde wire within the aorta during retrograde PCI for CTO, particularly in cases with difficult coronary engagement of the GC such as ostial occlusion, coronary anomaly, or GC mismatch.
Of note, the snare described above is not suitable for intracoronary use and therefore does not replace small snares for retrieval of foreign bodies inside the coronary arteries.
Tips and tricks for use
For setting up the homemade snare, various PCI balloons are suitable as long as their size exceeds the inner diameter of the GC. Our snare system consists of devices used in every PCI and does not require other special material. In rare cases, the wire lumen of the balloon collapses during inflation, rendering wire movement impossible. Therefore, we recommend an initial functional test of the constructed snare system outside of the body.
To avoid vessel injury, selection of a soft GW is preferable. Using the floppy part at the tip of the GW further improves safety and stands in contrast to a previously reported homemade snare using the stiff shaft of a 300 cm GW for the snare loop5. In case of difficulties in advancing the retrograde GW tip into the snare loop, the GC should be pulled back and the snare loop enlarged until it is attached to the aortic wall. This wide size adjustability offers an advantage for successful snaring. In cases of snaring the stiffer shaft (rather than the softer tip) or a generally stiff retrograde wire, its re-straightening within the GC might be impossible, thus the kinked retrograde wire cannot be pulled out from the retrograde microcatheter. In such particular cases other applicable techniques such as the “pull-through” technique7 should be selected.
Clinical experience
We present a case of a 49-year-old obese (body mass index: 33.3 kg/m2) female patient with dyslipidaemia (on statin) and ischaemia on exercise treadmill test. A coronary angiogram revealed a total coronary occlusion at the ostium of the left main trunk (LMT) and good collateral flow from the RCA (Figure 4). A left ventriculogram showed a preserved ejection fraction of 54%. Due to the patient’s preference for a minimally invasive procedure, PCI for LMT was scheduled.
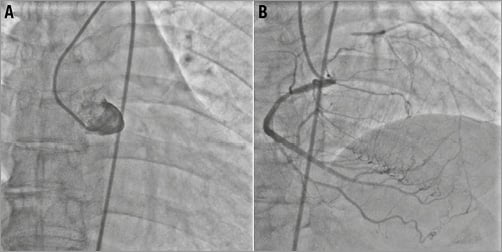
Figure 4. Representative case. Initial coronary angiogram (CAG) showed a total coronary occlusion at the ostium of the LMT (A) with good collateral flow from the right coronary artery (RCA) (B).
Due to the abrupt, stumpless CTO located at the ostium of the LMT, a retrograde approach was selected. After administration of 10,000 units of heparin, the RCA was engaged with a 6 Fr GC via the right radial artery. A Suoh wire (ASAHI Intecc, Aichi, Japan), supported by a FineCross™ MG micro-guide catheter (Terumo Corp., Tokyo, Japan) was advanced to the left anterior descending artery (LAD) through a septal channel (Figure 5A). Finally the CTO could be crossed retrogradely using a Fielder guidewire (ASAHI Intecc) (Figure 5B).
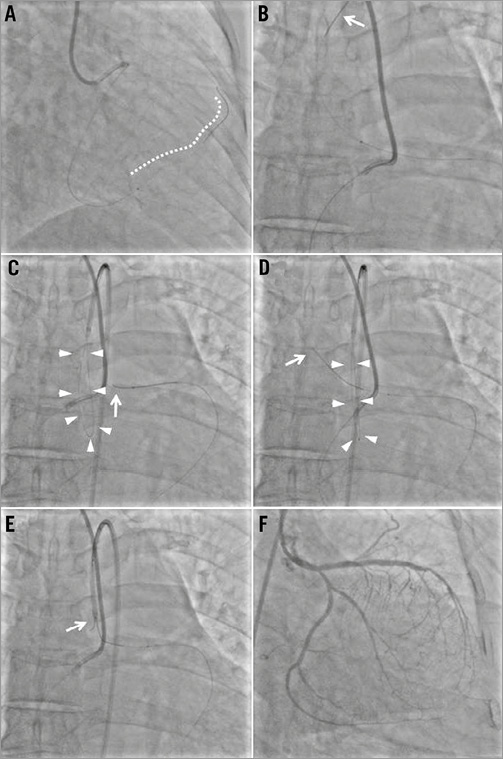
Figure 5. Representative case (contd). A Suoh wire (ASAHI Intecc) supported by a FineCross micro-guide catheter (Terumo Corp.) was advanced from the right coronary artery through a septal channel to the left anterior descending artery (LAD) (A). Using a Fielder guidewire (ASAHI Intecc) the CTO could be crossed retrogradely into the aorta (B). Through a 6 Fr GC (EBU 3.5) the homemade snare was placed in the ascending aorta. Once the retrograde wire tip was caught by the homemade snare it could be pulled into the antegrade GC (E). After the retrograde wire was exchanged for a long wire for externalisation, the LMT and LAD could successfully be revascularised using two drug-eluting stents.
Common externalisation of the retrograde GW failed due to the location of the CTO in the ostial LMT and the resulting inability to advance the retrograde GW into the antegrade GC. Consequently, snaring the retrograde GW using a homemade snare was performed.
A 6 Fr EBU 3.5 catheter (Medtronic, Minneapolis, MN, USA) was placed in the ascending aorta (Figure 5C). Made of a previously used Runthrough® NS GW (Terumo Corp.) and a 2.0 mm balloon catheter, the snare was unfolded in the aorta. The retrograde GW (Fielder) was advanced into the snare loop (Figure 5D). After catching the retrograde GW tip (Figure 5E, Moving image 1) the retrograde microcatheter (FineCross) could be advanced into the antegrade GC. The retrograde GW (Fielder) was released from the snare by deflating the balloon and pulling out the snare system. Finally, the retrograde GW (Fielder) was exchanged for a 300 cm RG3 wire (ASAHI Intecc). Following wire externalisation, the LMT could be revascularised successfully by implanting two drug-eluting stents. A final angiogram showed an optimal result with no vascular complications (Figure 5F).
| Impact on daily practice Snaring is not often used in daily practice but it can be an important procedure. Because of infrequent use, prepared snare devices in the cathlab are limited and not always suitable for the situation. Our novel snare consists of devices in daily use: a GC, a PCI balloon, and a 0.014” GW. It is safe, easy, economical and size-adjustable, and can be applied to catch a retrograde wire or a foreign body. |
Conflict of interest statement
Satoru Sumitsuji received honoraria from Terumo Corp., Medtronic, ASAHI Intecc. Shinsuke Nanto received honoraria from Medtronic Corp. The other authors have no conflicts of interest to declare.
Online data supplement
Moving image 1. A Fielder guidewire (ASAHI Intecc) succeeded in crossing the CTO retrogradely into the aorta. Through a 6 Fr GC (EBU 3.5) the homemade snare was placed in the ascending aorta. Once the retrograde wire tip was caught by the homemade snare it could be pulled into the antegrade GC.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1.
