A 28-year-old woman with recurrent episodes of respiratory infections, haemoptysis and an empyema was diagnosed with intralobar pulmonary sequestration (Figure 1A, Moving image 1).
In order to diminish the risk of intraoperative bleeding, we used Amplatzer® devices (St. Jude Medical, St. Paul, MN, USA) as a prior step to surgery (Figure 1B, Figure 1C, Moving image 2, Moving image 3). We decided to use one device for each peripheral branch (Appendix Figure 1) in order to avoid difficulty when sectioning the main vessel. The surgery was carried out successfully without significant bleeding.
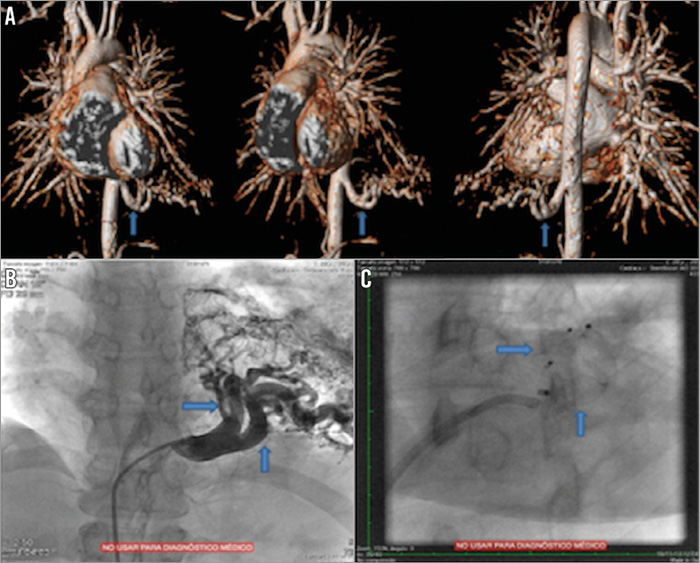
Figure 1. Magnetic resonance and angiography imaging. A) Magnetic resonance imaging reconstruction showing blood supply coming from a large-sized aortic dependent artery. B) & C) Angiography imaging before (B) and after (C) placing the Amplatzer devices.
The use of this device has been widely described to occlude cardiac and vascular abnormalities. It has also been used in the management of bronchial pleural fistulae, but this is the first description in a pulmonary sequestration.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Preoperative assessment showed blood supply. The drainage was through the pulmonary artery.
Moving image 2. Release of the Amplatzer device.
Moving image 3. End of the embolisation. We did not act on the non-occluded branch because of its size.

Appendix Figure 1. Specimen with both devices inside the two peripheral branches.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Preoperative assessment showed blood supply. The drainage was through the pulmonary artery.
Moving image 2. Release of the Amplatzer device.
Moving image 3. End of the embolisation. We did not act on the non-occluded branch because of its size.