Abstract
Background: In patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) and who are treated with direct oral anticoagulants (DOACs), dual antithrombotic treatment without aspirin is recommended. Evidence comparing P2Y12 inhibitor strategies in this setting is limited.
Aims: This study aimed to compare outcomes with ticagrelor versus clopidogrel as part of dual antithrombotic treatment in ACS patients undergoing PCI.
Methods: Using data from the SWEDEHEART registry, we conducted a cohort study including patients on dual antithrombotic treatment with ACS undergoing PCI between January 2014 and February 2022. Outcomes within one year were analysed using multivariate Cox regression to obtain adjusted hazard ratios (aHR) with 95% confidence intervals (CI) for major adverse cardiovascular events (MACE; including mortality, myocardial infarction [MI], and stroke), all-cause mortality, clinically relevant bleeding, and MI.
Results: A total of 3,708 patients were included (median age 76 years; 69% males; 40% ST-segment elevation myocardial infarction). At discharge, 1,170 (32%) received ticagrelor and 2,538 (68%) clopidogrel. For MACE, the unadjusted event rate was 16.7% in the ticagrelor group and 16.6% in the clopidogrel group (aHR 1.02, 95% CI: 0.84-1.23). Mortality occurred in 6.6% of patients treated with ticagrelor and 6.2% of those treated with clopidogrel (aHR 1.24, 95% CI: 0.91-1.69). Bleeding was 4.9% in the ticagrelor group compared with 3.7% in the clopidogrel group (aHR 1.53, 95% CI: 1.06-2.22). MI occurred in 10.4% of patients on ticagrelor and 11.2% of those on clopidogrel (aHR 0.90, 95% CI: 0.71-1.13).
Conclusions: In ACS patients on DOACs undergoing PCI, ticagrelor was associated with an increased risk of bleeding compared with clopidogrel, with no differences in MACE, mortality, or MI.
Patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) are typically treated with dual antiplatelet therapy, consisting of aspirin and a P2Y12 inhibitor. However, approximately 10% of these patients also require direct oral anticoagulant (DOAC) therapy, most commonly due to atrial fibrillation.1 This subgroup presents a unique challenge as they are at an increased risk of bleeding, raising the critical question of the optimal antithrombotic strategy after PCI.
Compared with triple antithrombotic treatment, three randomised controlled trials (RCTs) have reported that dual antithrombotic treatment, combining a P2Y12 inhibitor with a DOAC but without aspirin, reduces the risk of bleeding and is comparable in terms of ischaemic events.234 Another randomised controlled trial reported non-inferiority with dual antithrombotic treatment regarding bleeding compared with triple antithrombotic treatment and similar rates of ischaemic events.5 Consequently, both European and North American guidelines recommend dual antithrombotic treatment in these patients, with clopidogrel being the preferred P2Y12 inhibitor.67 However, in patients receiving dual antithrombotic treatment, comparative evidence evaluating different P2Y12 inhibitors is limited.
Clopidogrel is a prodrug requiring activation via the polymorphic cytochrome P450 isoenzyme CYP2C19; it is dosed once daily and binds irreversibly to the P2Y12 receptor. Ticagrelor does not require activation, is dosed twice daily, and binds reversibly to the P2Y12 receptor.8 Patients with reduced function of CYP2C19 treated with clopidogrel are reportedly at increased risk of major adverse cardiovascular events (MACE).9 Furthermore, reduced pharmacodynamic effects of clopidogrel have been reported for patients with diabetes mellitus type two and patients with a high body mass index (BMI).101112
Thus, our hypothesis was that greater platelet inhibition with ticagrelor compared with clopidogrel may improve outcomes in patients on dual antithrombotic treatment. As far as we are aware, no study has directly compared clinical outcomes between the P2Y12 inhibitors ticagrelor and clopidogrel in the context of dual antithrombotic treatment without aspirin for ACS patients requiring concurrent DOAC therapy. The aim of this study was therefore to investigate this issue in patients with ACS undergoing PCI.
Methods
In this cohort study, patient outcomes were compared one year after an ACS event with PCI between patients being prescribed ticagrelor and a DOAC, and patients being prescribed clopidogrel and a DOAC. The study was approved by the Swedish Ethical Review Authority (2023-00201-01).
Data were obtained from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR), the Register of Information and Knowledge about Swedish Heart Intensive Care Admissions (RIKS-HIA), the Swedish Prescribed Drug Register, and the Swedish National Patient Register (NPR). All these registries are nationwide. SCAAR contains data from coronary angiographies and PCI procedures, with a coverage of 98.1% in 2020.13 RIKS-HIA contains data regarding ACS from all hospitals with a cardiac intensive care unit.14 The Swedish Prescribed Drug Register records all prescriptions filled in pharmacies in Sweden.15 Through the NPR, diagnoses from inpatient care, according to the International Classification of Diseases-10 (ICD-10), are obtainable.16 The data were linked using the unique Swedish personal identity number.17
The following variables were extracted from SCAAR: year of index ACS event, BMI, smoking status, sex, previous coronary artery bypass grafting, diabetes mellitus, previous PCI, antithrombotic treatment during PCI, complete revascularisation, multivessel disease, non-ST-segment elevation myocardial infarction (NSTEMI), ST-segment elevation myocardial infarction (STEMI), unstable angina, proximal infarction in coronary segments, ≥2 stents used during PCI, and death. From RIKS-HIA, data regarding medications at discharge were extracted. From the Swedish Prescribed Drug Register, data regarding filled prescriptions both prior to and after the event were extracted. From the NPR, we extracted diagnoses that had been recorded, from inception to the index date: previous bleeding, cancer, chronic obstructive pulmonary disease, dementia, dialysis, heart failure, hypertension, previous myocardial infarction (MI), kidney failure, peripheral vessel disease, and stroke. A four-item PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Antiplatelet Therapy (PRECISE-DAPT) score was calculated from the data from SCAAR, NPR, and RIKS-HIA.18 The corresponding ICD-10 and ICD-9 codes are presented in Supplementary Table 1.
In the present study, we included the first-time event of an ACS treated with PCI in patients being prescribed a DOAC and ticagrelor or clopidogrel at discharge from January 2014 to February 2022. Follow-up data until 15 February 2022 were available. Patients who did not survive until discharge were not included in the study population. Those discharged with aspirin were excluded. The index date was defined as the date of the PCI. The P2Y12 inhibitor at discharge defined the group.
Outcomes within one year from the index date included MACE, all-cause mortality, bleeding, MI, stroke, and stent thrombosis. MACE was defined as a composite of all-cause mortality, MI, and stroke. Bleeding was defined as readmissions with the ICD codes shown in Supplementary Table 1, including intracranial haemorrhage, anaemia secondary to acute blood loss, gastrointestinal bleeding, iron deficiency anaemia due to chronic blood loss, ocular haemorrhage, otorrhagia, genitourinary bleeding, haemoptysis, airway haemorrhage, and postoperative or procedure-related bleeding. The MI outcome included readmissions with the ICD codes shown in Supplementary Table 1, including acute MIs and acute myocardial reinfarctions. Stent thrombosis was defined as definite stent thrombosis verified by coronary angiography.
To account for treatment adherence, patients were censored at 14 days post-discharge if no prescription for a DOAC nor the P2Y12 inhibitor they were treated with at discharge had been filled within this time, provided also that no such prescription had been filled before the event, as the patients could otherwise have already had a supply of the drug at home. Additionally, patients were censored if the treatment was switched, defined as the date of filling a prescription for the other P2Y12 inhibitor or for aspirin.
Statistical analysis
Data management and statistical analysis were performed using the programming language R, version 4.3.1 (R Foundation for Statistical Computing). Differences between the comparison groups were investigated using the Wilcoxon rank-sum test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. A p-value<0.05 was defined as statistically significant.
In the main analysis, Cox regression was used to calculate crude and adjusted hazard ratios (HRs). The adjustment model was determined a priori and included age, BMI, sex, smoking status, year of index ACS event, previous bleeding, diabetes, heart failure, hypertension, kidney failure, previous myocardial infarction, previous stroke, STEMI, and PRECISE-DAPT score. A total of 437 patients (11.8%) had missing information regarding at least one variable included in the multivariate model and were subsequently excluded from the multivariate analyses. The proportionality of hazards assumption was tested by visual inspection of the Kaplan-Meier curves (Supplementary Figure 1). In exploratory subgroup analyses, we calculated the p-value for interaction across characteristics regarding age, BMI, prior bleeding, kidney failure, sex, diabetes, PRECISE-DAPT score, previous MI, smoking status, and STEMI. Subgroups were assessed for MACE using the same adjustment model as in the main analysis. In a second subgroup analysis of bleeding, due to frequent event counts <5 per covariate, only crude HRs were reported to avoid overfitting.19 In the main analysis, the same approach was applied for the outcomes of stroke and stent thrombosis, where event counts were similarly low.
Two sensitivity analyses with differing levels of censoring were conducted: one without censoring based on filled prescriptions and another with additional censoring based on the planned duration of the P2Y12 inhibitor treatment at discharge. A sensitivity analysis restricted to major bleeding was performed in the same manner as the main analyses, using readmissions coded with the ICD diagnoses listed in Supplementary Table 1, including intracranial haemorrhage, anaemia due to acute blood loss, and gastrointestinal bleeding. Additionally, sensitivity analyses using inverse probability of treatment weighting (IPTW) with stabilised weights were performed based on propensity scores estimated through multivariate logistic regression, incorporating the same covariates used in the main analyses. These analyses were conducted for the outcomes of MACE, all-cause mortality, bleeding, and MI. After applying IPTW, covariate balance between groups was considered adequate if the mean difference was <0.1. The distribution of weights was evaluated using histograms.
Results
Patient characteristics
A total of 3,708 patients were included in the analyses (Figure 1); 1,170 (32%) were prescribed ticagrelor and 2,538 (68%) clopidogrel. The median age of the study population was 76 years, the median BMI was 26.7 kg/m2, 69% were males, 13% were smokers, and 14% had diabetes mellitus (Table 1, Supplementary Table 2). Regarding the index event, 40% had STEMI, 48% had NSTEMI, and 12% had unstable angina. Regarding DOACs at discharge, 70% had apixaban, 19% had rivaroxaban, 9% had dabigatran, and 2% had edoxaban. The percentage of patients receiving ticagrelor as part of dual antithrombotic treatment varied between 15% and 48% during the years of the study period (Figure 2).
Patients treated with ticagrelor, compared with those treated with clopidogrel, were younger and had a higher BMI (Table 1, Supplementary Table 2). Furthermore, the prevalence of smoking, diabetes mellitus, and STEMI was higher in the ticagrelor group. Conversely, the prevalence of prior bleeding events as well as heart and kidney failure was lower in the ticagrelor group, as was the median PRECISE-DAPT score.
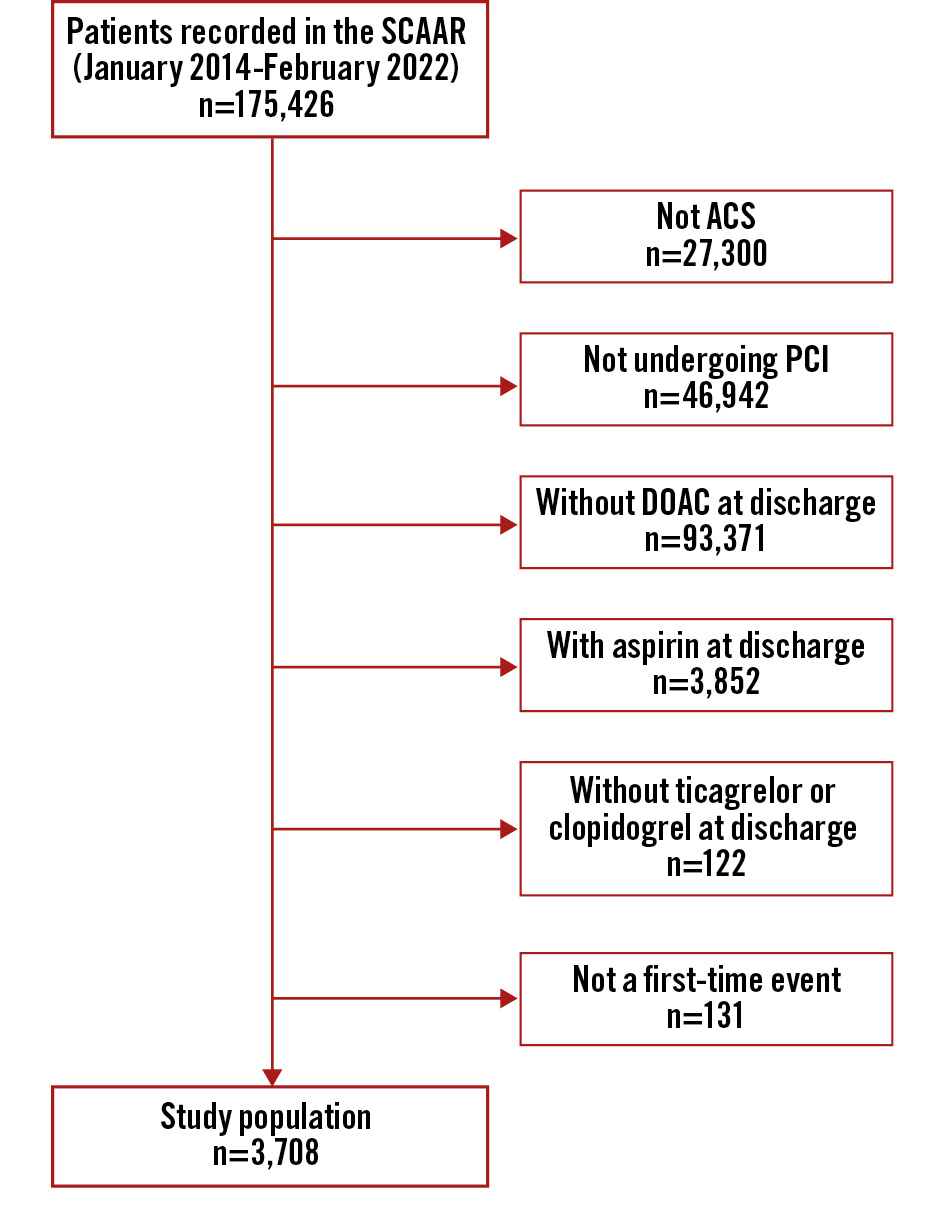
Figure 1. Flowchart of the study population. ACS: acute coronary syndrome; DOAC: direct oral anticoagulant; PCI: percutaneous coronary intervention; SCAAR: Swedish Coronary Angiography and Angioplasty Registry
Table 1. Characteristics of the compared groups.
| Ticagrelor n=1,170 | Clopidogrel n=2,538 | Unknown | p-value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 74 (67-80) | 77 (71-83) | 0 (0) | <0.001 |
| BMI, kg/m2 | 27.1 (24.3-30.5) | 26.5 (24.1-29.7) | 106 (2.9) | 0.007 |
| Smoker | 180 (16) | 281 (12) | 166 (4.5) | <0.001 |
| Male sex | 813 (69) | 1,732 (68) | 0 (0) | 0.45 |
| Year of the index ACS event | ||||
| 2014 | 7 (0.6) | 14 (0.6) | 0 (0) | <0.001 |
| 2015 | 65 (5.6) | 71 (2.8) | ||
| 2016 | 106 (9.1) | 131 (5.2) | ||
| 2017 | 169 (14) | 214 (8.4) | ||
| 2018 | 210 (18) | 287 (11) | ||
| 2019 | 225 (19) | 388 (15) | ||
| 2020 | 239 (20) | 557 (22) | ||
| 2021 | 140 (12) | 825 (33) | ||
| 2022 | 9 (0.8) | 51 (2.0) | ||
| Previous medical history | ||||
| Bleeding | 80 (6.8) | 225 (8.9) | 0 (0) | 0.037 |
| CABG | 110 (9.4) | 252 (9.9) | 1 (<0.1) | 0.62 |
| Cancer | 60 (5.1) | 150 (5.9) | 0 (0) | 0.34 |
| COPD | 111 (9.5) | 265 (10) | 0 (0) | 0.37 |
| Dementia | 5 (0.4) | 23 (0.9) | 0 (0) | 0.12 |
| Diabetes mellitus | 223 (19) | 302 (12) | 0 (0) | <0.001 |
| Dialysis | 2 (0.2) | 8 (0.3) | 0 (0) | 0.73 |
| Heart failure | 157 (13) | 454 (18) | 0 (0) | <0.001 |
| Hyperlipidaemia | 560 (49) | 1,350 (54) | 66 (1.8) | 0.005 |
| Hypertension | 831 (72) | 1,952 (78) | 36 (1.0) | <0.001 |
| Kidney failure | 52 (4.4) | 202 (8.0) | 0 (0) | <0.001 |
| MI | 315 (27) | 799 (32) | 65 (1.8) | 0.003 |
| Peripheral vessel disease | 93 (7.9) | 215 (8.5) | 0 (0) | 0.59 |
| PCI | 300 (26) | 724 (29) | 0 (0) | 0.068 |
| Stroke | 107 (9.1) | 303 (12) | 0 (0) | 0.012 |
| Clinical characteristics | ||||
| Complete revascularisation | 719 (63) | 1,619 (65) | 78 (2.1) | 0.20 |
| Multivessel disease | 601 (51) | 1,321 (52) | 0 (0) | 0.70 |
| STEMI | 520 (44) | 963 (38) | 0 (0) | <0.001 |
| NSTEMI | 522 (45) | 1,242 (49) | 0 (0) | 0.014 |
| Unstable angina | 128 (11) | 333 (13) | 0 (0) | 0.061 |
| PRECISE-DAPT score | 14 (10-20) | 17 (13-25) | 186 (5.0) | <0.001 |
| Proximal infarction | 560 (48) | 1,169 (46) | 0 (0) | 0.31 |
| ≥2 stents used during PCI | 416 (36) | 937 (37) | 0 (0) | 0.42 |
| Values are presented as n (%) or median (25th-75th percentile). BMI: body mass index; CABG: coronary artery bypass graft; COPD: chronic obstructive pulmonary disease; MI: myocardial infarction; NSTEMI: non-ST-segment elevation myocardial infarction; PCI: percutaneous coronary intervention; PRECISE-DAPT: PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual AntiPlatelet Therapy; STEMI: ST-segment elevation myocardial infarction | ||||
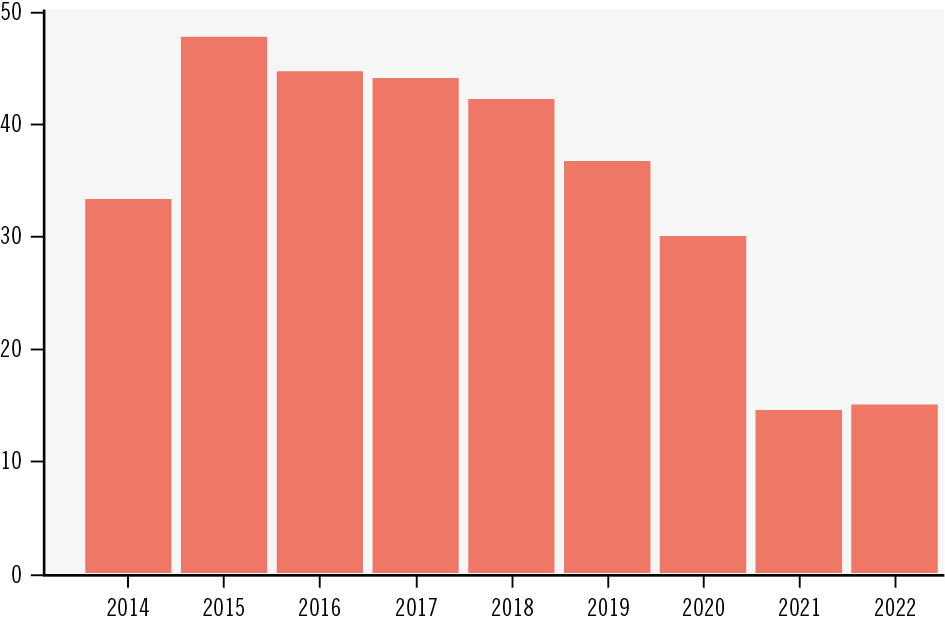
Figure 2. Percentage of the study population discharged with ticagrelor from 2014 to 2022.
Outcomes
For MACE, the ticagrelor and clopidogrel groups experienced unadjusted 16.7% and 16.6% event rates, respectively, with an adjusted hazard ratio of 1.02 (95% confidence interval [CI]: 0.84-1.23) (Table 2, Central illustration). Unadjusted mortality rates were 6.6% with ticagrelor versus 6.2% with clopidogrel, with an adjusted hazard ratio of 1.24 (95% CI: 0.91-1.69). Bleeding occurred in 4.9% of patients taking ticagrelor compared with 3.7% in the clopidogrel group, with an adjusted hazard ratio of 1.53 (95% CI: 1.06-2.22). MI was observed in 10.4% of the ticagrelor group versus 11.2% in the clopidogrel group, with an adjusted HR of 0.90 (95% CI: 0.71-1.13). For stroke and stent thrombosis, the rates were 1.4% versus 1.2% and 0.3% versus 0.4%, respectively, for ticagrelor versus clopidogrel, and no significant differences were found.
Table 2. Number of events post-censoring for all the outcomes within one year.
| Ticagrelor n=1,170 | Clopidogrel n=2,538 | Hazard ratio (95% CI) | ||
|---|---|---|---|---|
| Crude | Adjusteda | |||
| MACE | 195 (16.7) | 422 (16.6) | 0.97 (0.82-1.15) | 1.02 (0.84-1.23) |
| Mortality | 77 (6.6) | 157 (6.2) | 1.02 (0.78-1.34) | 1.24 (0.91-1.69) |
| Bleeding | 57 (4.9) | 93 (3.7) | 1.30 (0.94-1.81) | 1.53 (1.06-2.22) |
| MI | 122 (10.4) | 285 (11.2) | 0.90 (0.73-1.12) | 0.90 (0.71-1.13) |
| Stroke | 16 (1.4) | 31 (1.2) | 1.06 (0.58-1.93) | Too few events |
| Stent thrombosis | 3 (0.3) | 11 (0.4) | 0.55 (0.15-1.97) | Too few events |
| Data are n (%). aAdjusted for age, body mass index, sex, smoking, year of the index ACS event, previous bleeding, diabetes, heart failure, hypertension, kidney failure, previous myocardial infarction, previous stroke, ST-segment elevation myocardial infarction, and PRECISE-DAPT score. CI: confidence interval; MACE: major adverse cardiovascular events; MI: myocardial infarction; PRECISE-DAPT: PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual AntiPlatelet Therapy | ||||
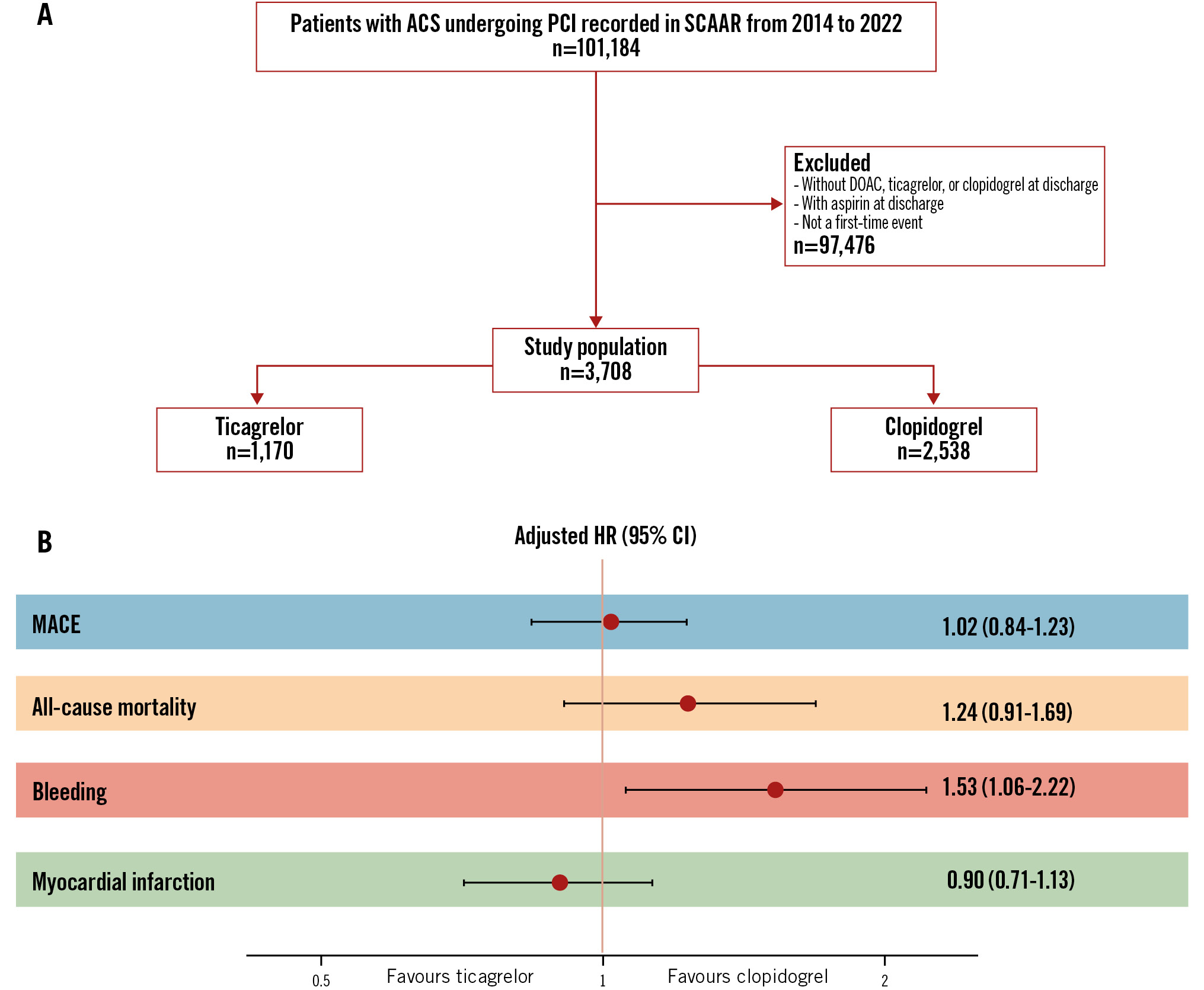
Central illustration. Comparison of ticagrelor versus clopidogrel in orally anticoagulated patients with ACS undergoing PCI without aspirin. A) Study flowchart; (B) forest plot for clinical outcomes. ACS: acute coronary syndrome; CI: confidence interval; DOAC: direct oral anticoagulant; HR: hazard ratio; MACE: major adverse cardiovascular events; PCI: percutaneous coronary intervention; SCAAR: Swedish Coronary Angiography and Angioplasty Registry
Subgroup analyses
In subgroup analyses with MACE as the dependent variable, no statistically significant interaction was found regarding age, BMI, prior bleeding, kidney failure, sex, diabetes mellitus, PRECISE-DAPT score, previous MI, or smoking status (Figure 3). A statistically significant interaction was observed between STEMI status and treatment effect on MACE. Among patients with STEMI, ticagrelor was associated with a non-significant trend towards reduced MACE rates, whereas in patients without STEMI, a non-significant trend towards increased MACE rates was noted. In unadjusted subgroup analyses with bleeding as the outcome, significant interactions were observed, accompanied by non-significant trends suggesting a potentially increased bleeding risk with ticagrelor in patients aged ≥75 years, with a BMI <30 kg/m2, without a history of prior bleeding, and whose index ACS event was not classified as STEMI (Supplementary Figure 2). Due to the limited number of bleeding events, adjusted analyses could not be performed.
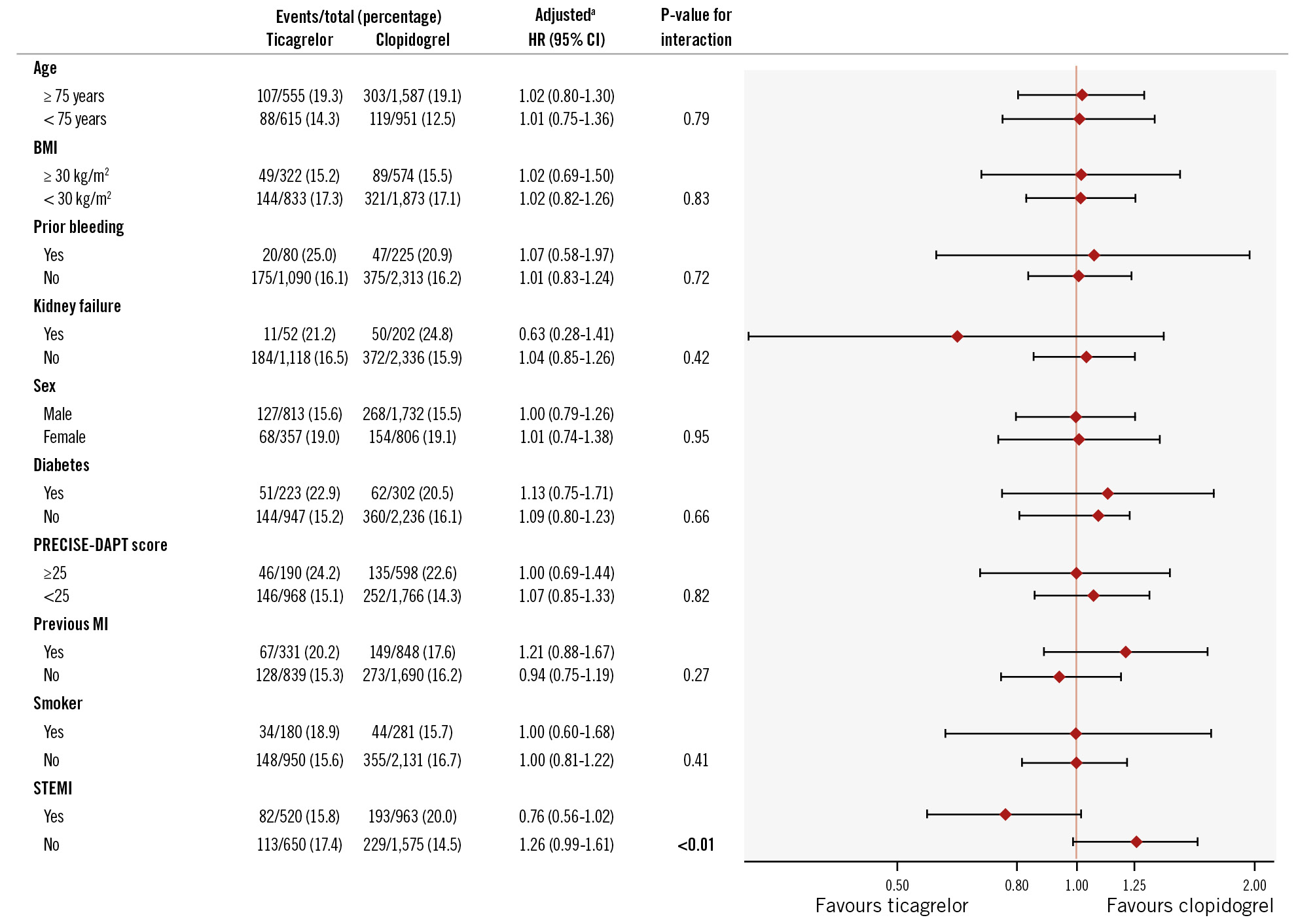
Figure 3. Number of MACE per subgroup within one year of the index ACS event and adjusted hazard ratios with 95% CI and p-values for interaction. The p-value in bold is statistically significant. aAdjusted for age, body mass index, sex, smoking, year of the index ACS event, previous bleeding, diabetes, heart failure, hypertension, kidney failure, previous myocardial infarction, previous stroke, ST-segment elevation myocardial infarction, and PRECISE-DAPT score. ACS: acute coronary syndrome; BMI: body mass index; CI: confidence interval; HR: hazard ratio; MACE: major adverse cardiovascular events; MI: myocardial infarction; PRECISE-DAPT: PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual AntiPlatelet Therapy; STEMI: ST-segment elevation myocardial infarction
Sensitivity analyses
Sensitivity analyses without censoring, and with additional censoring based on the planned treatment time with P2Y12 inhibitors, showed results similar to the main results (Supplementary Table 3, Supplementary Table 4). In a sensitivity analysis focusing solely on major bleeding, 35 patients (3.0%)treated with ticagrelor experienced an event compared with 48 (1.9%) treated with clopidogrel, yielding an adjusted HR of 1.63 (95% CI: 0.95-2.80) and a p-value of 0.077. In the sensitivity analysis using IPTW, all covariates were balanced between the comparison groups, and no extreme weights were observed (median weight [interquartile range]: 0.92 [0.82-1.11]; minimum: 0.44; maximum: 3.79) (Supplementary Figure 3, Supplementary Figure 4). The results were similar to those from the main analyses (Supplementary Table 5).
Discussion
In patients with ACS undergoing PCI and treated with a DOAC, ticagrelor – compared with clopidogrel – was not significantly associated with a favourable effect on the risk of MACE, all-cause mortality, MI, stroke, or stent thrombosis after adjustments for baseline characteristics. Thus, our hypothesis that greater platelet inhibition with ticagrelor would improve outcomes in these patients was not confirmed. On the contrary, ticagrelor was associated with a 53% higher hazard of bleeding.
Our results regarding MACE are consistent with a previous unadjusted analysis showing no difference between ticagrelor and clopidogrel regarding the odds of MACE.20 Exploratory subgroup analyses for MACE revealed a non-statistically significant trend towards a benefit in patients with STEMI but with a significant p-value for interaction. Patients with STEMI, as they tend to have a higher thrombus burden,21 may represent a more thrombogenic cohort.22 Therefore, one could speculate that patients with STEMI would benefit from more potent platelet inhibition at discharge than those without STEMI. However, since the results from the subgroup analyses are primarily exploratory and hypothesis-generating, this result would need further confirmation in an RCT. The non-statistically significant trend towards a higher rate of MACE in patients without STEMI remains unclear. Residual confounding cannot be excluded. Interestingly, diabetes and obesity were not identified as effect modifiers, despite previous associations with clopidogrel resistance in these populations.101112
Regarding bleeding, our results demonstrating an associated increased risk of bleeding are consistent with a previously published unadjusted analysis reporting 52% higher odds of bleeding.20 Furthermore, these results align with previous literature indicating that ticagrelor, compared with clopidogrel, may increase the risk of bleeding.23 Interestingly, the ticagrelor group had a lower prevalence of characteristics associated with a higher risk of bleeding, such as lower age, prior bleeding, kidney failure, stroke, and a lower PRECISE-DAPT score. Thus, patients with a lower risk of bleeding seem more often to be prescribed ticagrelor. Residual confounding cannot be excluded, and one may speculate that such bias would make the association even more pronounced. Indeed, the crude HR implied a statistically non-significant 30% increase, whereas the adjusted HR showed a statistically significant 53% increase. Furthermore, exploratory subgroup analyses revealed that age, BMI, prior bleeding, and STEMI were effect modifiers. However, the number of events were too few to allow for adjusted analyses, and the findings carry a substantial risk of confounding. Nevertheless, it has previously been shown in patients treated with dual antiplatelet therapy that older age is associated with an increased risk of bleeding with ticagrelor versus clopidogrel, with non-inferiority shown for the net clinical benefit.24 In the sensitivity analysis restricted to major bleeding, we observed a non-statistically significant trend towards a higher bleeding risk associated with ticagrelor compared with clopidogrel, with an adjusted HR that was similar to that of the main analysis. One could speculate that the non-statistically significant result may reflect a lack of statistical power as there were 45% fewer bleeding events in this analysis compared with the main analysis.
Overall, our results are consistent with current European and North American guidelines from 2024 and 2025, respectively, which recommend clopidogrel as the preferred choice of P2Y12 inhibitor.67 Interestingly, European guidelines from 2016 and 2020 as well as North American guidelines from 2018 and 2021 also recommend clopidogrel as the preferred choice.25262728 As our study only includes patients with ACS, it remains uncertain whether our findings can be extrapolated to patients with stable angina undergoing PCI. However, a subgroup analysis of an RCT in patients with atrial fibrillation undergoing PCI reported that a less intensive antithrombotic regimen consisting of dual therapy with a P2Y12 inhibitor and dabigatran was favoured over triple therapy with warfarin, a P2Y12 inhibitor, and aspirin, in both ACS and elective procedure settings.29 These results may suggest that for both those with ACS and elective PCI, reducing antithrombotic intensity could be beneficial. In addition, current European guidelines recommend a less potent antiplatelet strategy in patients with stable angina compared with those presenting with ACS, reflecting the lower thrombotic risk in this group.3031 Taken together, these observations could support the hypothesis that our results, which indicate a beneficial association of less intensive antithrombotic treatment with clopidogrel compared with ticagrelor in orally anticoagulated patients with ACS who are not treated with aspirin, may also extend to patients with stable angina undergoing PCI. Nonetheless, such interpretations should be made with caution: dedicated studies in this population are lacking. Interestingly, in an RCT investigating non-orally anticoagulated ACS patients, prasugrel was reported to be superior to ticagrelor regarding MACE, but with similar rates of bleeding.32 As our data included few patients who were treated with prasugrel, we focused on ticagrelor versus clopidogrel. Thus, whether our results extend to prasugrel remains unknown. Future investigations evaluating prasugrel in this patient population would be of interest.
A key strength of the present study is the use of nationwide registry data, which enhances generalisability by reflecting outcomes in routine clinical practice across an entire population. Furthermore, our registry data include important variables that enable us to take crucial aspects into account in adjustment models. Additional strengths include that the sensitivity analyses with differing amounts of censoring, as well as the IPTW analysis, demonstrated that the main results were robust.
Limitations
Limitations include the fact that the comparison groups differed in terms of several characteristics, and even if adjustments were made to account for these differences, residual confounding cannot be excluded. Additionally, information regarding some important aspects was not available in our data, such as the clinical indication for the treatment with a DOAC, drug dosages, and the patients’ CYP2C19 function. Furthermore, we had to assume that the P2Y12 inhibitor prescribed at discharge reflected the P2Y12 inhibitor prescribed during the initial admission. Another limitation of our study is that the data required to calculate the most recent score, the PRECISE-High Bleeding Risk score,33 were not available, and the PRECISE-DAPT score had to be used instead. Moreover, a standardised bleeding classification could not be applied to our bleeding outcome, because our data lack information on haemoglobin and haematocrit decline, as well as documentation of the haemodynamic consequences of the bleeding.34 Finally, the number of bleeding events were too few to allow for adjusted subgroup analyses.
Conclusions
In ACS patients on DOACs undergoing PCI, ticagrelor was associated with a higher bleeding risk compared with clopidogrel, with no favourable associations regarding the risks of MACE, mortality, or MI.
Impact on daily practice
In this nationwide Swedish registry-based study, we conducted, to our knowledge, the first direct comparison of ticagrelor and clopidogrel in patients with acute coronary syndrome undergoing percutaneous coronary intervention and receiving treatment with a direct oral anticoagulant, without aspirin. We observed no difference in ischaemic outcomes, and ticagrelor was associated with an increased risk of bleeding (adjusted hazard ratio 1.53). These findings are consistent with current guidelines, describing clopidogrel as the preferred P2Y12 inhibitor in these patients.
Funding
This article was funded by Skåne University Hospital funds (SUS stiftelser och fonder), the Swedish Research Council, and the Swedish Heart Lung Foundation, grant number 20220432.
Conflict of interest statement
S. Koul declares speaker fees from Chiesi Farmaceutici and AstraZeneca. D. Erlinge has received honoraria for advisory board/speaker fees from Amgen, AstraZeneca, Chiesi, Sanofi, Novo Nordisk, InfraredX/Nipro, and Kaminari Medical. O. Braun has received honoraria for advisory board/speaker fees from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Novartis, Novo Nordisk, and Pfizer. T. Jernberg reports institutional grants from MSD; and a consultation fee from Amgen. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.