Introduction
The most common approach for coronary or carotid catheterisation or intervention is via the groin1,2. However, in some elderly patients catheter manipulation via the femoral approach is barred by a high level of friction due to severe kinking of the iliac artery, most probably because of atherosclerotic vessel remodelling3.
A common solution is to use a larger, rigid, kink-resistant long sheath with a stiff guidewire. Nevertheless, in rare cases the kinking cannot be overcome and the friction remains so high that the investigator has to puncture the contralateral side or switch to the transradial approach, which might also be extremely difficult because the atherosclerotic disease is often generalised.
Indications for use
The parallel sheath technique from the femoral route is indicated in cases of severe tortuosity of the access arteries that prevent acceptable manoeuvrability of catheters and devices. It will dramatically reduce friction and will thus make it much easier to continue the diagnostic or interventional procedure. We do not recommend using closing devices after the end of the procedure.
Tips and tricks for delivery
Once the decision has been made to insert a second sheath you should keep a catheter and a stiff 0.035” wire in the first sheath and puncture 1-2 mm medially (sometimes laterally), aiming towards the palpable sheath. In most cases this is easier than the first puncture. If it fails, you may puncture assisted by fluoroscopy. It appears appropriate to use a 4 Fr sheath and a 4 Fr diagnostic catheter for straightening the artery with the second 0.035” guidewire.
Description
We describe five cases of considerable kinking of the iliac artery in which conventional transfemoral techniques, including larger kink-resistant sheaths and extra-support guidewires, failed to allow sufficient steerability to engage the diagnostic and guiding catheters properly. The common bail-out technique for all cases was to insert a second sheath close to the first into the same common femoral artery to facilitate manoeuvrability of catheters and wires by straightening the tortuous access with two extra-stiff 0.035” wires.
CASE 1
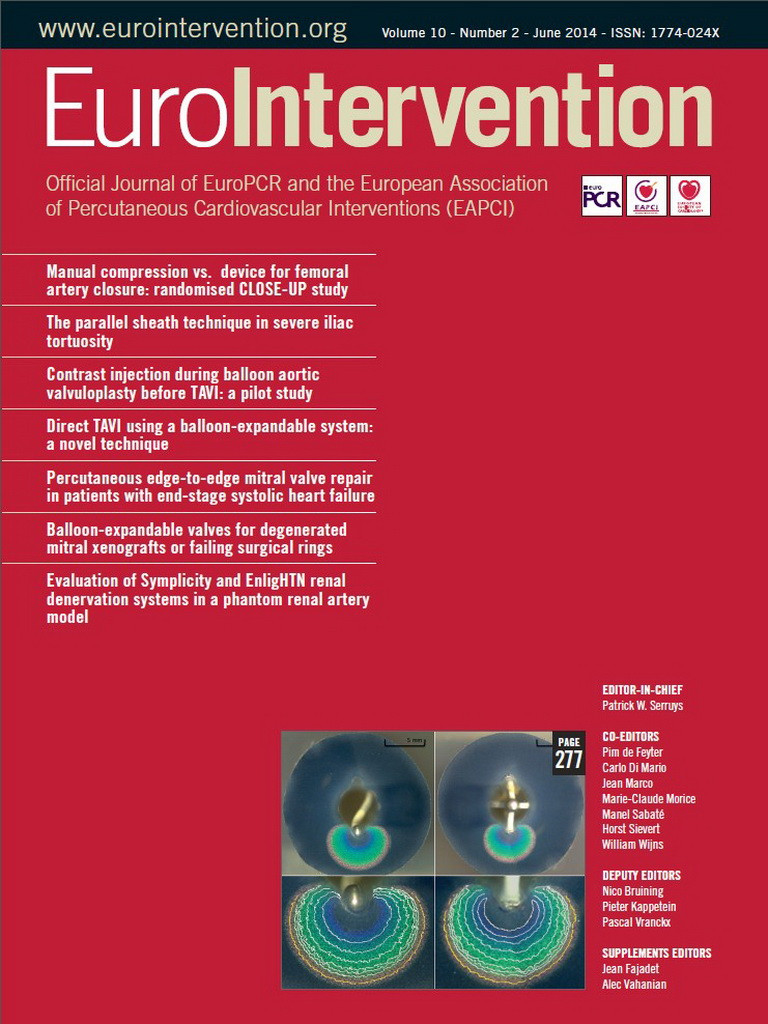
A 79-year-old male with an 80% stenosis of the right common carotid artery which was due for carotid artery stenting. In this case even advancing the 5 Fr diagnostic catheter via the right groin was not possible although we used a long kink-resistant 8 Fr Arrow 45 cm sheath (Teleflex Medical, Athlone, Ireland) and a 0.035 inch extra-stiff Amplatz® guidewire (Cook Medical, Bloomington, IN, USA) which straightened the artery considerably. However, despite straightening, the friction was so tight that we were unable even to advance the 5 Fr catheter beyond the abdominal aorta (Figure 1A). We therefore decided to switch to the left groin, but experienced an even worse iliac kinking, so that we decided to work from the right side again. This time we inserted a second long 5 Fr Arrow 45 cm sheath parallel to the 8 Fr sheath that had remained in place, and advanced a stiff Back-up Meier™ 0.035 inch guidewire (Boston Scientific, Natick, MA, USA) via the 5 Fr sheath, nicely straightening the artery. We were then able easily to advance and manipulate the 5 Fr and 8 Fr catheters via the 8 Fr sheath without any friction using a regular 0.035 inch guidewire (Figure 1B). The common carotid artery was then successfully dilated and stented.
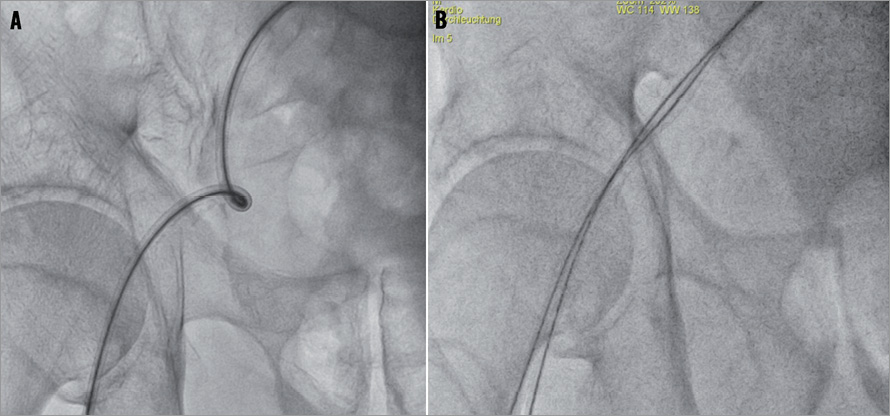
Figure 1. A) Right iliac artery kinking despite 8 Fr Arrow 45 cm sheath (Teleflex Medical) and a 0.035” extra-stiff Amplatz® guidewire (Cook). A diagnostic 5 Fr catheter was unable to be advanced beyond the abdominal aorta because of excessive friction. B) A second long 5 Fr Arrow 45 cm sheath parallel to the 8 Fr sheath and a stiff Back-up Meier 0.035” guidewire (Boston Scientific) via the 5 Fr sheath straightened the artery. The angiography and intervention were finished successfully without major friction.
CASE 2
A 73-year-old male with three-vessel coronary artery disease, coronary artery bypass grafting (CABG) 17 years ago, progressive angina pectoris CCS IV. In spite of severe iliac kinking and considerable friction, the diagnostic coronary angiography with 5 Fr catheters was achieved using the right groin, a kink-resistant long 5 Fr sheath and a 0.035 inch extra-stiff Amplatz® guidewire (Cook Medical), revealing 50% stenosis of the left main coronary artery, an 80% lesion of the proximal left anterior descending coronary artery (LAD) and occlusions of the right coronary artery (RCA) and circumflex coronary artery (CX), both supplied by collaterals from the LAD. Bypass grafts to RCA, CX and LAD were occluded.
PCI of the last remaining vessel, the LAD, was strongly indicated. The 5 Fr sheath was exchanged for a 7 Fr 45 cm kink-resistant Arrow sheath (Teleflex Medical) (Figure 2A), but the guiding catheter could not be advanced over the 0.035 inch extra-stiff Amplatz® guidewire (Cook Medical) because of severe friction. We inserted a second 5 Fr Arrow 45 cm sheath parallel to the 7 Fr sheath into the same artery. After inserting a stiff Back-up Meier 0.035 inch guidewire (Boston Scientific) through this 5 Fr sheath the vessel was straightened (Figure 2B) and we were then able to complete the intervention successfully without any friction via the 7 Fr sheath. Rapid and secure manipulation was crucial since the patient experienced severe angina and blood pressure drop at each balloon inflation.
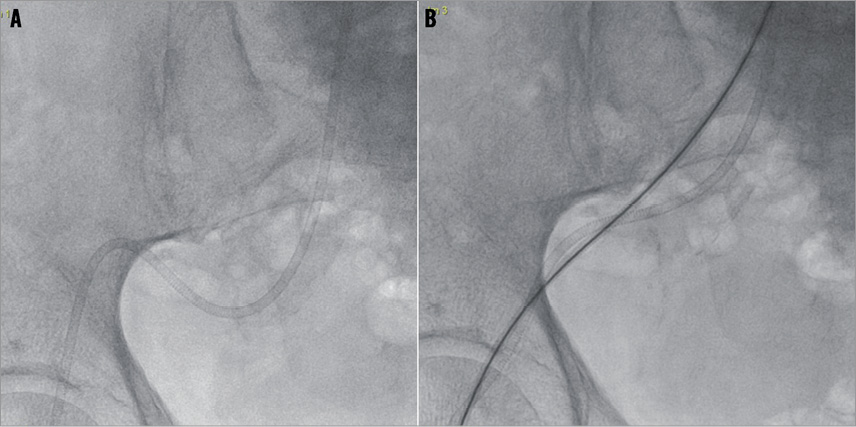
Figure 2. A) A 7 Fr 45 cm kink-resistant Arrow sheath (Teleflex Medical). B) A second 5 Fr Arrow 45 cm sheath with a stiff Back-up Meier 0.035” guidewire (Boston Scientific) straightened the artery and the intervention was finished successfully without major friction.
CASE 3
A 71-year-old male with hip dysplasia. Coronary angiography was indicated prior to hip surgery because ECG and echocardiography suggested relevant coronary artery disease. Coronary angiography was initially impossible because of serious elongation and kinking of the iliac artery (Figure 3A), resulting in insuperable friction of the 5 Fr diagnostic catheter over a 0.035 inch extra-stiff Amplatz® guidewire (Cook Medical) in a long 5 Fr Arrow (Teleflex Medical) sheath. Finally, we inserted a second long 5 Fr Arrow 45 cm sheath parallel to the first and replaced the Amplatz 0.035 inch guidewire by a stiff Back-up Meier 0.035 inch guidewire (Boston Scientific) (Figure 3B) which then allowed catheterisation without any friction. Coronary angiography revealed two-vessel coronary artery disease with no indication for revascularisation prior to hip surgery.
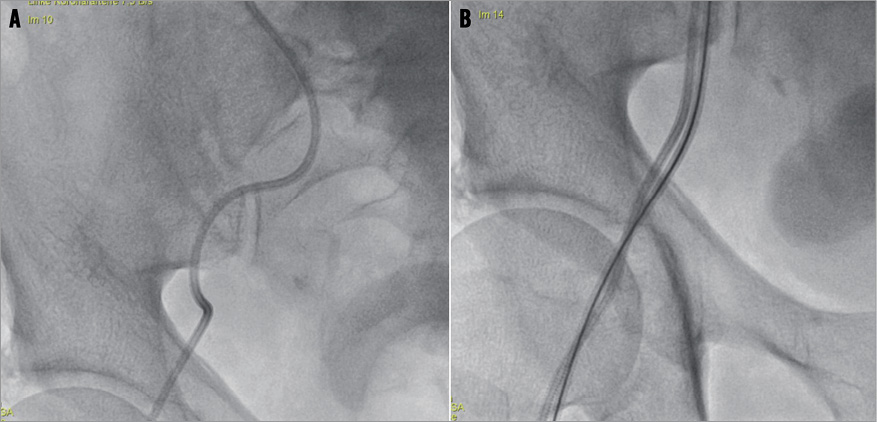
Figure 3. A) Long 5 Fr Arrow (Teleflex Medical) sheath in a severe kinking of the right iliac artery. B) Two long 5 Fr Arrow sheaths with a stiff Back-up Meier 0.035” guidewire (Boston Scientific).
CASE 4
A 75-year-old male with three-vessel coronary artery disease post CABG 14 years ago complained of progressive dyspnoea NYHA Class II. We suspected relevant progression of the coronary artery disease and planned a coronary angiography. Due to massive whorls of the artery and severe friction it was impossible to manoeuvre the catheter (Figure 4A). The friction was reduced dramatically and the angiography was performed easily only after parallel insertion of two 45 cm kink-resistant Arrow sheaths (5 Fr and 6 Fr; Teleflex Medical) and a Back-up Meier 0.035 inch guidewire (Boston Scientific) (Figure 4B). Prognostically relevant progression of the coronary artery disease was ruled out.
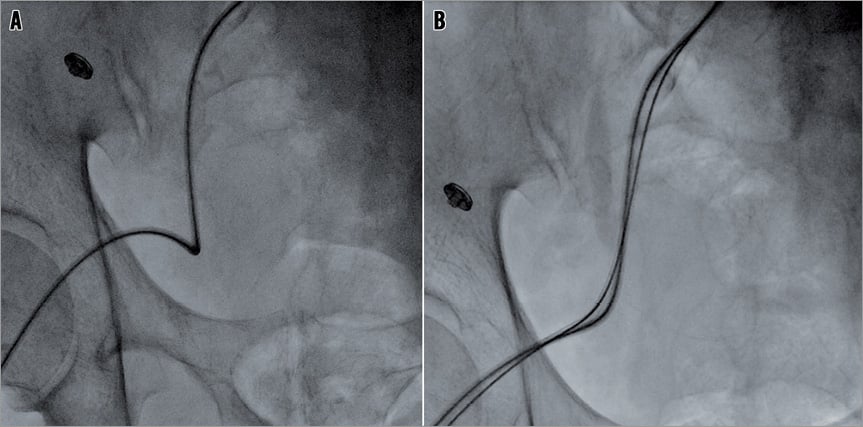
Figure 4. A) A 5 Fr 45 cm kink-resistant Arrow sheath (Teleflex Medical) insufficiently straightened with a 0.035” extra-stiff Amplatz® guidewire (Cook). B) One 5 Fr and one 6 Fr Arrow 45 cm sheath with a stiff Back-up Meier™ 0.035” guidewire (Boston Scientific) straightened the artery and the angiography was performed easily without major friction.
CASE 5
A 74-year-old hypertensive male patient with symptomatic obstruction of the right superficial femoral artery. A crossover manoeuvre via the left groin was impossible because of severe kinking of the ipsilateral iliac artery in spite of a kink-resistant 7 Fr sheath (Arrow; Teleflex Medical) and an extra-stiff 0.035 inch guidewire (Figure 5). Only after inserting a second 4 Fr sheath in the same groin and further straightening the iliac artery with a second stiff 0.035 inch guidewire (Back-up Meier; Boston Scientific) within a 4 Fr diagnostic catheter was crossover wiring and stenting of the SFA successful.
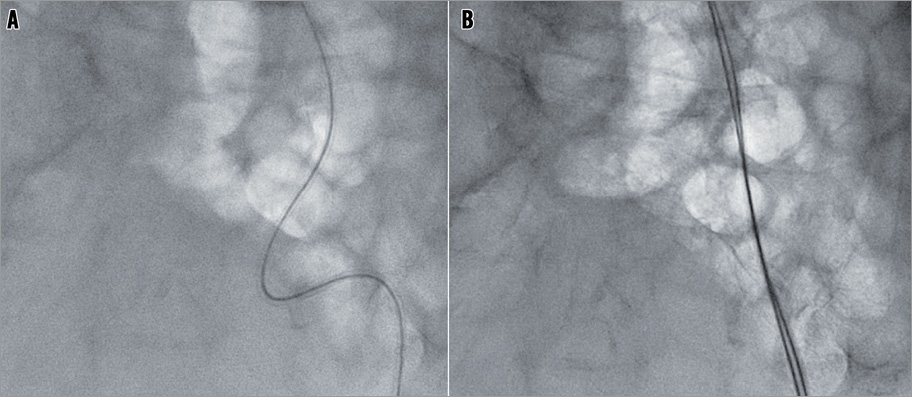
Figure 5. A) A 7 Fr 45 cm kink-resistant Arrow sheath (Teleflex Medical) insufficiently straightened with a 0.035” extra-stiff Amplatz® guidewire (Cook). B) An additional 4 Fr sheath (Terumo Corp., Tokyo, Japan) and a stiff Back-up Meier™ 0.035” guidewire (Boston Scientific) within a 4 Fr diagnostic catheter straightened the artery and the crossover manoeuvre and intervention of the right SFA were performed easily without major friction.
In all cases the sheaths were removed immediately and the groin compressed manually, keeping a bandage on for six hours without any bleeding complications.
Conclusions
In the presence of severe tortuosity and atherosclerosis of the femoral or iliac arteries, catheterisation and interventions via the femoral access might be impossible, even via long kink-resistant sheaths and stiff guidewires. The insertion of a second arterial sheath parallel to the first and the straightening of the iliac artery with an extra-stiff wire will considerably ease manipulation via the first sheath.
Discussion
To our knowledge this is the first report of a simple and novel parallel sheath technique to improve steerability markedly in situations of insuperable femoral or iliac kinking.
In general, operators try to overcome these difficulties using an alternative access (left femoral or radial), which, however, might not be any easier. Other possible solutions are to select sheath sizes exceeding those of the guiding catheter, or to insert a small sheath into a big sheath4. However, these techniques are unable to overcome extreme friction and poor steerability sufficiently. Some operators suggest applying the “dental floss” technique5 where one places a stiff Glidewire (Terumo) through the brachial artery into the iliac artery. Once the tip of the wire is placed in the iliac artery, a long catheter can be inserted over the Glidewire into the iliac artery. The Glidewire is exchanged through the catheter for a Lunderquist wire (Cook Medical) that can then be grasped with a snare and brought out through the femoral artery. This technique also straightens tortuous iliac arteries, and is used mainly for endovascular repair of abdominal aortic aneurysms, but is not suitable for cardiac or carotid interventions that require meticulous catheter manipulation. Our simple novel technique of parallel sheaths has the advantage that the operator literally experiences no friction once the vessel is straightened with a parallel sheath and a stiff guidewire. Surprisingly, the rate of bleeding complications is not increased compared to single sheath insertion6. The parallel sheath technique has been applied by one of the authors (NR) since 2006 in more than 500 cases of patients with chronic coronary occlusion (7 Fr and 5 Fr or 6 Fr parallel sheaths) for contralateral injection or retrograde recanalisation approach with major in-hospital bleeding complications of <1%, defined as requirement of vascular surgery or transfusion of >1 blood unit6.
Conflict of interest statement
The authors have no conflicts of interest to declare.