A 39-year-old man was admitted to intensive care unit because of hypotension. Septic shock of unknown origin was suspected. All cultures were negative. The patient got worse and a new continuous murmur was heard by cardiac auscultation. Transthoracic (TTE) and transesophageal (TEE) echocardiography were performed. Echocardiography revealed an aorta-to-right atrial fistula due to the rupture of a non-coronary sinus aneurysm, without images compatible with infective endocarditis (Figures 1A and 1B). Transcatheter occlusion with an Amplatzer device was decided and performed without complications (Figures 1C and 1D) improving patient’s clinical condition.
One week after, the patient developed heart failure and TTE was performed. It revealed an acute severe aortic regurgitation due to prolapse of the non-coronary aortic leaflet that did not previously exist (Figure 1E). The patient did not have episodes of fever and there was no evidence of infective endocarditis in the TTE images. He underwent aortic valve replacement. Native aortic valve culture was negative and the surgeon noted that there was no macroscopic evidence of infection or inflammation (Figure 1F). Aortic regurgitation was explained as the consequence of the mechanical interference of the Amplatzer with the leaflet causing its prolapse, due to the weight of the device. The patient was finally discharged 15 days after an uneventful postoperative period.
Aortic regurgitation due to the interference of the device with aortic leaflets has been described as a possibility in the literature1 but, to the best of our knowledge; it is the first time that it has been demonstrated.
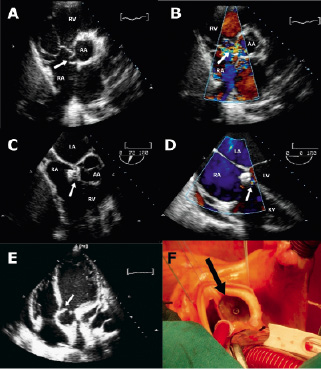
Figure 1. A. Transthoracic echocardiography, short axis view: the fistula (arrow) between ascending aorta (AA) and right atrium (RA) is patent. B. Transthoracic echocardiography, short axis view, colour-Doppler flow imaging: there is a systolic turbulent flow (arrow) through the fistula between aorta (AA) and right atrium (RA). C. Transesophageal echocardiography after Amplatzer device implantation, mid-oesophageal view in a 75º plane: the device (arrow) has been deployed correctly. D. Transesophageal echocardiography after Amplatzer device implantation, mid-oesophageal view in a 0º plane, colour-Doppler flow imaging: there is a little shunt (arrow) beside the Amplatzer duct occluder device. E. Transthoracic echocardiography, apical 4-chamber view: prolapse of the non-coronary aortic leaflet (arrow). F. Photograph taken in operating theatre showing the Amplatzer device (arrow) without signs of infection and that is not endothelised. RA: right atrium; LA: left atrium; RV: right ventricle; LV: left ventricle
Reference
Online data supplement
Video 1. Transesophageal echocardiography, mid-oesophageal view in a 75º plane: The fistula between ascending aorta and right atrium is shown.
Video 2. Transesophageal echocardiography, mid-oesophageal view in a 75º plane, colour-Doppler flow imaging: There is a systolic turbulent flow through the fistula between aorta and right atrium.
Video 3. Transesophageal echocardiography after Amplatzer device implantation, mid-oesophageal view in a 75º plane: The device has been deployed correctly.
Video 4. Transthoracic echocardiography, zoom of an apical 4-chamber view: prolapse of the non-coronary aortic leaflet.
