Occlusion of the left atrial appendage (LAA) by an LAA occluder (LAAO) has become an alternative treatment to oral anticoagulants for stroke prevention in patients with atrial fibrillation1. However, device-related thrombus might occur because of incomplete endothelialisation of the LAAO surface2. Current imaging techniques, such as transoesophageal echocardiography or computed tomography (CT), have limitations in detecting LAAO endothelialisation. Optical coherence tomography (OCT) has been widely used in coronary intervention procedures for the visualisation of plaque morphology, stent apposition and stent endothelialisation3. In the present study, we proposed a technique for evaluating LAAO endothelialisation using OCT images.
As this was a first-in-human procedure, we proposed performing it in conjunction with pulmonary vein isolation in eligible patients with a pre-existing LAAO. Pulmonary vein isolation was performed first using the three-dimensional (3D)-mapping system and a steerable sheath, as in our previously reported methods45.
After transseptal puncture, we inserted a transseptal sheath through a percutaneous transvenous mitral valvuloplasty (PTMV) Inoue wire (Toray) to prevent the catheter tip damaging the left atrium (LA). As mentioned above, we performed PVI first, using a steerable catheter and an irrigated-tip ablation catheter5. After PVI, we carried out the OCT study using the same steerable catheter. First, the steerable catheter was advanced close to the LAAO device. Then, we inserted a 6 Fr Judkin right 4 (JR4; Medtronic) guiding catheter (GC) into the LA, via the steerable sheath, and manipulated the GC even closer to the LAAO device.
We used the Dragonfly Opstar Catheter (Abbott) for the OCT study. The distal tapered plastic tip of the OCT probe was cut to expose the infrared probe and to facilitate the probe getting close to the device surface (Figure 1A). We then inserted a 0.014 inch coronary guidewire through the OCT catheter into the LA, and the OCT catheter was advanced over the wire to the LAAO device under fluoroscopic guidance.
The lateral aspect of the infrared probe should be very close to the LAAO surface in order to obtain high-quality images (Figure 1B). We manually injected contrast medium via the GC, and OCT images were recorded with a steady OCT probe on the LAAO surface, without pulling back. During the whole procedure, the activated clotting time was kept at >300 sec using heparin. The patients did not discontinue their antithrombotic agents for this procedure.
High-quality OCT images were obtained for both the WATCHMAN (Boston Scientific) and Amplatzer Amulet (Abbott) devices. An endothelialisation layer could be clearly appreciated on both the WATCHMAN and Amulet devices (Figure 1C, Figure 1D). The endothelialisation layer on the Amulet was generally thicker than on the WATCHMAN.
We have provided the procedural details of using OCT to visualise endothelialisation of LAAO and we have demonstrated the excellent quality of OCT for this procedure. However, performing post-LAAO OCT is invasive, and the procedural risks could overwhelm the benefits of this approach. Therefore, non-invasive tools, such as CT or magnetic resonance imaging, should still be utilised to clearly depict the surface of the device, and OCT should not be used solely for LAAO endothelialisation evaluation but, rather, as an adjuvant procedure, such as concomitantly with a pulmonary vein isolation procedure.
OCT is an invasive procedure despite the high-quality images it produces. OCT is also an excellent tool for device thrombus evaluation, although this was not carried out in the present study. Using OCT for viewing the entire surface of large LAAO would be a technical challenge. However, we advocate that a dedicated OCT catheter could be invented.
We describe a feasible procedure for visualising the endothelialisation of LAAO using a coronary OCT catheter.
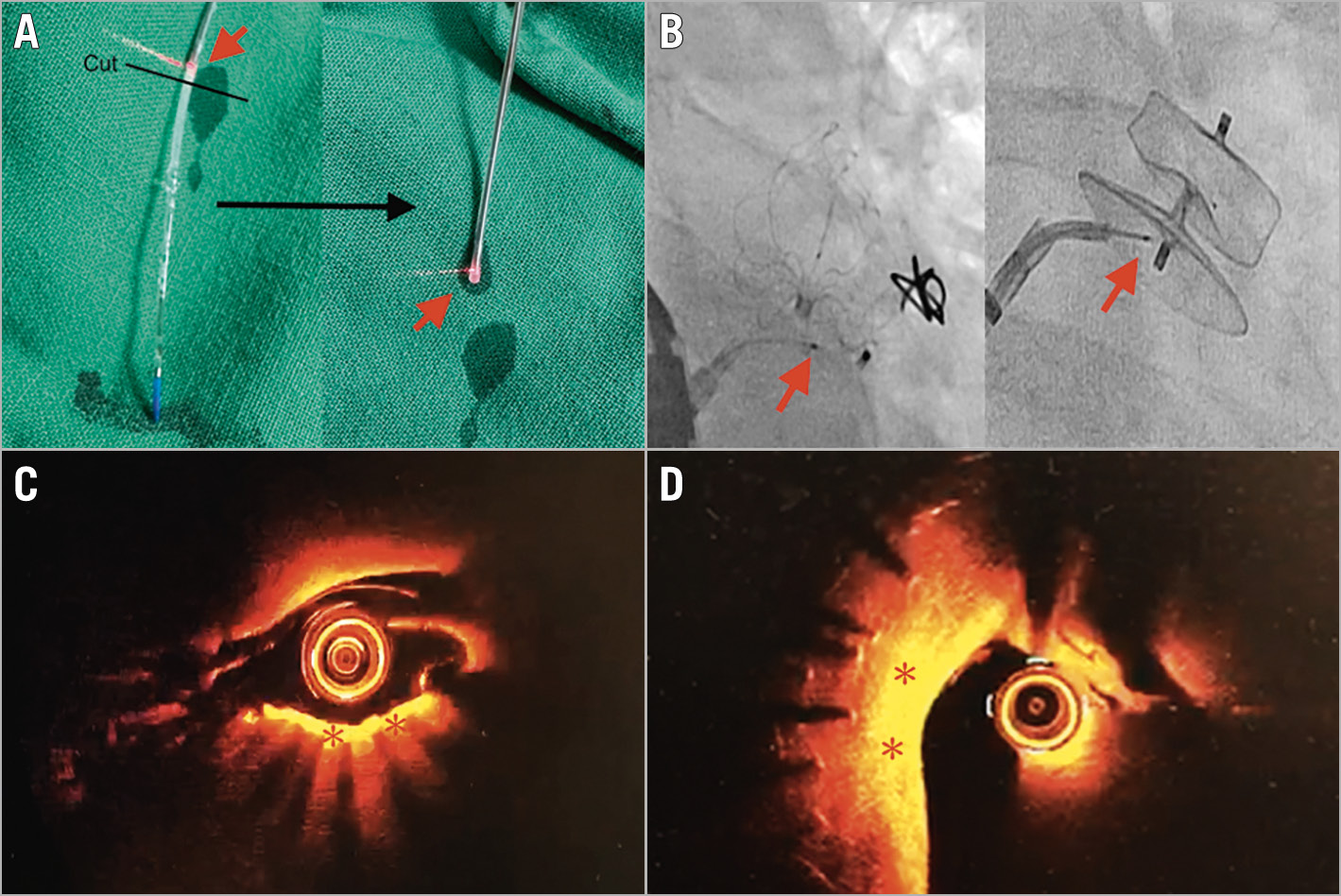
Figure 1. OCT images of LAAO endothelialisation. A) The distal OCT plastic tip was cut (black line) to expose the infrared OCT probe (red arrows). B) The OCT probe (red arrows) should be very close to the LAAO surface (left: WATCHMAN; right: Amulet). C) OCT shows endothelialisation of the WATCHMAN device (red asterisks). D) OCT shows endothelialisation of the Amulet device (red asterisks). LAAO: left atrial appendage occluder; OCT: optical coherence tomography
Conflict of interest statement
The authors have no conflicts of interest to declare