Abstract
Aims: Although preliminary experience has shown the feasibility of tricuspid valve clipping, intraprocedural guidance remains a major issue. The aim of this report is to provide a simple nomenclature for intraprocedural 3D TEE guidance during transcatheter tricuspid valve interventions.
Methods and results: The identification of the location of the aortic valve (AV) is fundamental to understanding the orientation of the leaflets: the leaflet opposite the AV is the posterior leaflet (P). Anterior (A) and septal (S) leaflets are easily identified counterclockwise. The movements of the guiding catheter in the right atrium can be divided for orientation: towards the AV (“Aortic” direction) or towards the posterior leaflet (“Posterior” direction); the movement perpendicular to the previous one can be towards the anterior (“Anterior” direction) or towards the septal leaflet (“Septal” direction).
Conclusions: We have provided a simple nomenclature, which can be shared between the person performing the procedure and the person who is guiding, that could serve as a “Rosetta Stone” for TV clipping, and for transcatheter TV interventions in general.
Tricuspid regurgitation (TR) is a common finding in patients with left-sided valvular heart disease and in patients with chronic heart failure, and it is associated with poor quality of life and increased mortality1. Transcatheter treatment of TR has recently emerged as an alternative to surgery for patients deemed to be at high risk, as well as for the compassionate treatment of highly symptomatic patients refractory to medical therapy. Different transcatheter devices are currently under preliminary clinical evaluation to treat functional TR (FTR), which represents the most frequent aetiology of TR2. Among them, transcatheter edge-to-edge repair performed with the MitraClip® system (Abbott Vascular, Santa Clara, CA, USA) in the tricuspid position is quickly gaining popularity, since feasibility and efficacy have recently been reported using both the transjugular and the transfemoral approach3,4.
Although preliminary experience has shown the feasibility of tricuspid valve clipping, intraprocedural guidance remains a major issue, since in many patients the echocardiographic window for the tricuspid valve may be suboptimal and the procedural steps have not yet been standardised. Procedural guidance with 3D transoesophageal echocardiography (TEE) represents a fundamental tool to achieve procedural success. However, in many patients the quality of intraprocedural guidance can often be suboptimal, mainly depending on patient variability and individual echo window. Moreover, the three-leaflet configuration of the tricuspid valve (TV) precludes the visualisation of all the leaflets in the same view in conventional two-dimensional echo. This aspect contributes to the increased technical complexity of TV interventions. Often a combination of TEE, transthoracic echocardiography, and intracardiac ultrasound together with fluoroscopy is used to achieve satisfactory visualisation. A detailed intraprocedural imaging is not only of particular importance to guide the operator to the segment of the valve which represents the target for clipping, but also crucial to define the orientation of the clip and to assess leaflet insertion.
Since experience with tricuspidal clipping is still really preliminary, it is of crucial importance to define a common nomenclature in order to standardise procedural 3D TEE guidance. Exactly as for the MitraClip procedure, communication between echocardiographer and interventionalist is fundamental; therefore, all the operators involved in the procedure should “speak the same language”. This is even more important at this stage, since most of the operators (both interventionalists and echocardiographers) are used to the conventional MitraClip nomenclature in the mitral position (lateral vs. medial; anterior vs. posterior), and this can create some misunderstanding due to the fact that the mitral nomenclature is inappropriately adapted to the tricuspid valve (TV). The aim of this report is to provide a simple nomenclature, which should be shared between the person performing the procedure and the person who is guiding, that could serve as a “Rosetta Stone” for TV clipping, and for transcatheter TV interventions in general (Figure 1).
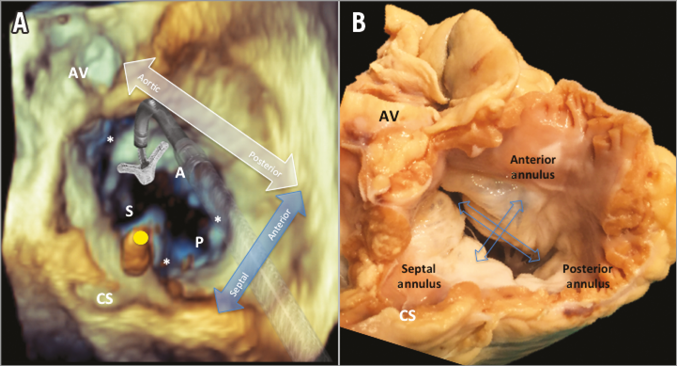
Figure 1. Proposed nomenclature. A) A 3D surgical view of the tricuspid valve during a tricuspid valve clipping. The MitraClip is delivered in the right atrium through the inferior vena cava. The yellow spot indicates a transvalvular pacemaker lead. B) A corresponding anatomical specimen of the tricuspid valve from a cadaveric human heart. Similar to the conventional MitraClip procedure, the identification of the location of the aortic valve (AV) is fundamental to understanding the orientation of the leaflets: the leaflet opposite the AV is the posterior leaflet (P). Anterior (A) and septal (S) leaflets are easily identified counterclockwise. The three stars (*) are located corresponding to the three commissures. The movements of the guiding catheter in the right atrium can be divided for orientation as illustrated: towards the AV (“Aortic” direction) by advancing the full system, or towards the posterior leaflet (“Posterior” direction) by retracting the full system; the movement perpendicular to the previous one can be towards the anterior (“Anterior” direction) or towards the septal leaflet (“Septal” direction). CS: coronary sinus
| Impact on daily practice The nomenclature provided, which can be shared between the person performing the procedure and the person who is guiding, could serve as a “Rosetta Stone” for TV clipping, and for transcatheter TV interventions in general. |
Conflict of interest statement
F. Maisano is a consultant for and receives research grants from Abbott Vascular. The other authors have no conflicts of interest to declare.