Abstract
Aims: The treatment of in-stent restenosis (ISR) remains challenging. Small case series have described successful utilisation of bioresorbable vascular scaffolds (BVS) (Absorb; Abbott Vascular, Santa Clara, CA, USA) to treat ISR. We report our experience with this novel approach.
Methods and results: Patients with ISR in native coronary arteries undergoing percutaneous coronary intervention (PCI) for ISR were treated using BVS. A total of 84 ISR lesions were treated in 65 patients. The mean age was 66±11 years, 28% had acute coronary syndrome (ACS) and 28% were diabetic. PCI was successful in all patients and all scaffolds were delivered and deployed successfully in the target lesion. All 65 patients had six-month follow-up and 49 patients had 12-month clinical follow-up. The target lesion revascularisation (TLR) rate was 3.1% at six months and 12.2% at 12 months. The mean duration from PCI to TLR was 301±148 days. No scaffold thrombosis occurred during the study period.
Conclusions: This proof of concept study demonstrates that ISR treatment utilising BVS is feasible and appears to have acceptable target lesion failure rates. Prospective randomised trials are necessary to assess whether BVS are more effective than drug-eluting stents or drug-eluting balloons to treat ISR.
Introduction
Although percutaneous coronary intervention (PCI) using drug-eluting stents (DES) has dramatically reduced the need for repeat intervention compared to bare metal stents (BMS)1, a substantial minority of patients still require reinterventions, and sometimes even coronary artery bypass grafting (CABG) needs to be considered in recurrent in-stent restenosis (ISR)2.
Drug-eluting balloons (DEB) are superior to plain old balloon angioplasty (POBA) when treating ISR3,4 but new-generation everolimus-eluting stents have been shown to be more effective than DEB when treating BMS5 and DES ISR6-8.
Implanting additional stent layers to treat ISR might be effective in the short term9, but the long-term consequences of more than two stent layers (“onion-skin phenomenon”) are unknown6. BVS offer a more prolonged drug delivery capacity and more radial strength in the acute phase. Additionally, compared to most DEB, the Absorb BVS (Abbott Vascular, Santa Clara, CA, USA) elutes everolimus, which is believed to be more effective in fighting restenosis when compared to paclitaxel10,11. Recent case reports and small series have suggested implantation of BVS to treat ISR, which might have positive effects on neoatherosclerosis and would avoid the addition of multiple metal layers12-14.
In this report, we describe our initial experience utilising BVS to treat ISR in an all-comers population with coronary artery disease (CAD).
Methods
STUDY POPULATION
This was an observational single-centre study which was performed at the Luzerner Kantonsspital (Lucerne, Switzerland), a centre performing 1,500 PCI/year by four operators. The Absorb BVS was introduced in July 2013 and, starting in September 2013, became optional to treat ISR. The final decision as to whether to use a DEB, DES or BVS for the treatment of ISR remained at the discretion of the interventional cardiologist. Patients with symptomatic stable CAD and those with acute coronary syndrome (ACS) were eligible to be treated using BVS. The interventional cardiology consultants agreed on the following exclusion criteria: previous stent thrombosis, restenosis in saphenous vein grafts or arterial grafts, vessel diameters <2.5 and >4.0 mm, large bifurcations requiring a two-stent strategy, and residual stenosis >50% after predilatation.
In the time period September 2013 to December 2014, a total of 84 other patients presented with ISR and were treated as follows: DES (n=62), DEB (n=14) and bypass surgery (n=8). The clinical and angiographic characteristics of these patients were largely comparable to those presented in this study.
TYPES OF STENT WITH ISR
The following stents had been used previously in the current population:
– BMS: PRO-Kinetic (Biotronik, Berlin, Germany, n=11); MULTI-LINK VISION® (Abbott Vascular, n=3).
– Early-generation DES: CYPHER® (Cordis, Johnson & Johnson, Fremont, CA, USA, n=15).
– Late-generation DES: XIENCE (Abbott Vascular, n=36); Orsiro (Biotronik, n=19).
Procedure
Predilatation was performed using non-compliant balloons from SIS Medical, Winterthur, Switzerland. Either the BEO NC® (highest rated burst pressure 24 atm) or the OPN NC® (highest rated burst pressure 35 atm) was used to predilate the ISR lesion. The Absorb BVS was implanted at 12-16 atm with gradually increasing pressure (as recommended) with the intention of covering the diseased segment completely. Post-dilatation was performed using the BEO NC and OPN NC. However, in the initial months, post-dilatation was performed only in selected cases. The strategy was then changed to post-dilate all BVS.
ANGIOGRAPHIC ANALYSIS AND OPTICAL COHERENCE TOMOGRAPHY
The angiographic pattern of ISR was classified in four categories according to Mehran et al15: focal (ISR <10 mm) diffuse (ISR >10 mm within the stent), proliferative (ISR >10 mm extending outside the stent) and occlusive (totally occluded ISR).
Quantitative angiographic analysis (QCA) was performed before (if the vessel was not completely occluded) and after BVS implantation using Xcelera software, Version 3.2.1 (Philips Healthcare, Best, The Netherlands). Measurements were taken on cineangiograms recorded after intracoronary nitroglycerine. Baseline measurements were taken with the single worst view projection and repeated in the same projection. The contrast-filled non-tapered catheter tip was used for calibration.
In selected cases optical coherence tomography (OCT) was used to guide BVS implantation. Angiographic and OCT images of a patient with ISR treated with BVS are shown in Moving images 1-7.
MEDICAL THERAPY
PCI was performed using heparin (70 units/kilogram body weight) and eptifibatide was used in selected patients with ACS (at the discretion of the operator). Patients with stable CAD were discharged on aspirin and clopidogrel whilst those with ACS received ticagrelor or prasugrel in addition to aspirin. As a general rule, dual antiplatelet therapy was recommended for 12 months.
FOLLOW-UP AND ENDPOINTS
Follow-up was performed via telephone or by clinical visits. Patients with re-occurrence of angina underwent invasive coronary angiography. The primary endpoint was a composite of target lesion revascularisation (TLR), scaffold thrombosis (ScT), myocardial infarction and death. Additionally, target vessel revascularisation (TVR) is reported.
Target lesion failure (TLF) was defined as re-occurrence of symptoms with angiographic diameter stenosis >50% at follow-up. ScT was defined according to the Academic Research Consortium definition16.
ETHICAL CONSIDERATIONS
All patients gave informed consent to be included in this registry and to be contacted regularly for clinical follow-up. This study was part of the preparation for the AbsorbISR study (a prospective, randomised study, ClinicalTrials.gov identifier: NCT02474485) and the institutional review board gave its approval.
Statistics
Normally distributed parameters are reported as mean and standard deviation (SD), and non-normally distributed parameters are reported as median (interquartile values). The paired and unpaired t-test was used for normally distributed parameters. A p-value <0.05 was considered significant.
Results
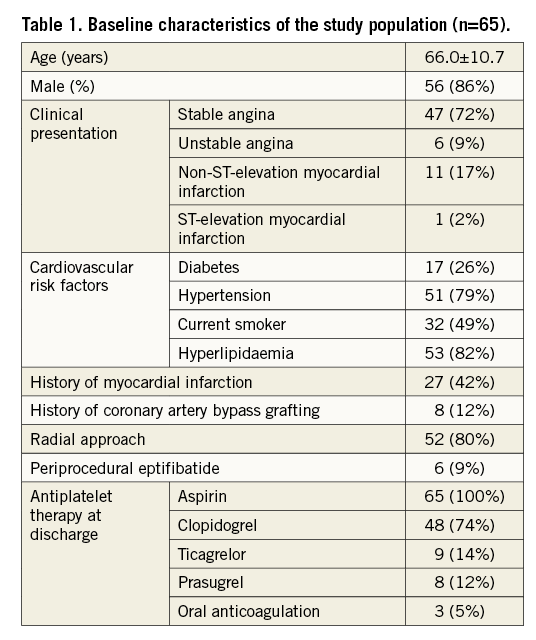
Between September 2013 and December 2014, a total of 84 ISR lesions were treated in 65 patients. The baseline characteristics of the study population are shown in Table 1. Briefly, the mean age was 66±11 years, 28% of the patients had ACS and 26% had diabetes mellitus. Patients with stable CAD were all symptomatic with angina CCS II or more.
LESION CHARACTERISTICS
The lesion characteristics are described in Table 2. The vast majority of the lesions were ISR in late-generation DES (71%). The rest were ISR lesions in early-generation DES (25%) and BMS (4%). Twenty-one lesions (29%) had two or more previous stents implanted and 17 lesions (20%) were chronic total occlusions.
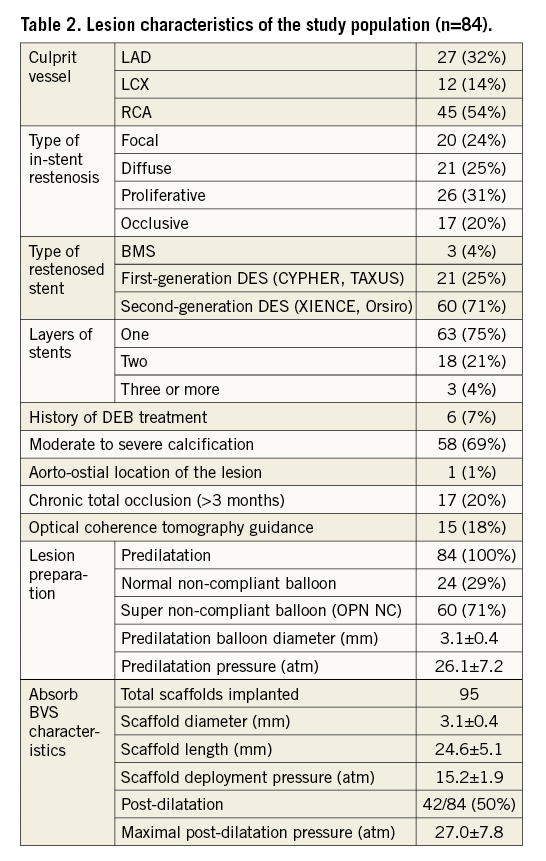
Predilatation was performed in all lesions and in all lesions a non-compliant balloon was used and inflated at high pressures, reaching a mean inflation pressure of 26±7 atm.
Procedure success was 100%, no major acute complication occurred and all scaffolds could be deployed to the target lesion. A total of 95 scaffolds were implanted with a mean diameter of 3.1±0.4 mm and a mean length of 24.6±5.1 mm. Mean deployment pressure was 15.2±1.8 atm and post-dilatation was performed in 42/84 lesions (50%). Mean post-dilatation pressure was 27.0±7.8 atm.
OCT was used in 15/84 lesions (18%). Post-dilatation pressure was similar in patients where OCT was used to guide the procedure (n=12) as compared to those in whom OCT was not used (n=27): 26.6±5.4 atm vs. 27.4±8.5 atm (p=0.77).
Figure 1 depicts the use of OCT to guide the procedure and to demonstrate endothelialisation of the scaffold at six months. Figure 2 demonstrates a patient with target lesion failure.
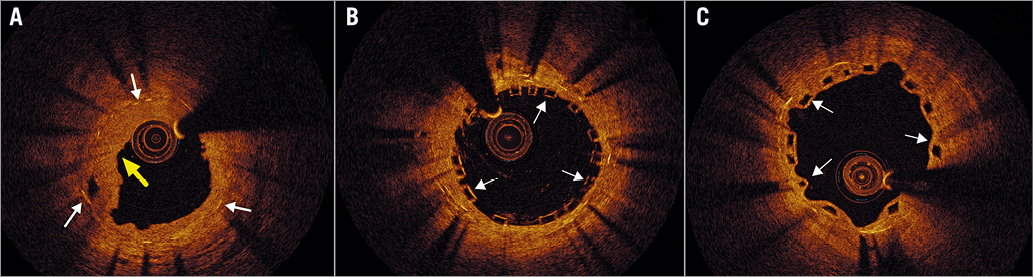
Figure 1. Optical coherence tomography images of a patient with in-stent restenosis treated with Absorb BVS. A) Baseline: optical coherence tomography demonstrates intimal hyperplasia covering a previously implanted drug-eluting stent (arrows). B) After BVS implantation: an Absorb BVS has been implanted achieving a good result with good scaffold expansion and apposition. C) At 6 months post PCI: the scaffold is covered by thin neointima but no in-stent restenosis is seen.
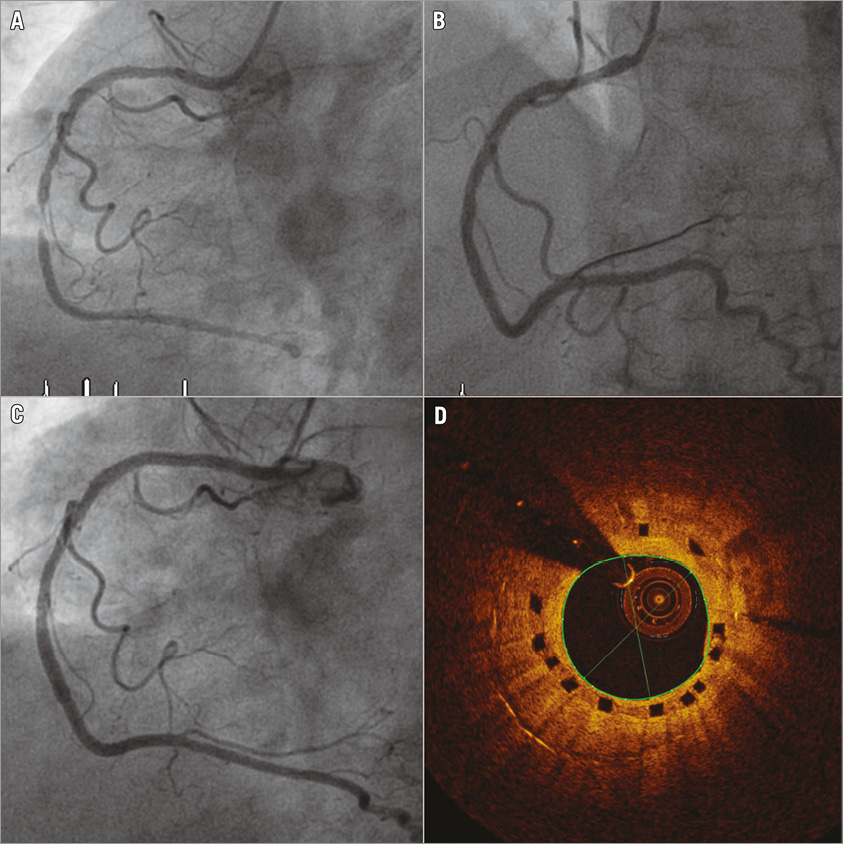
Figure 2. Angiographic and optical coherence tomography images in one of the patients with target lesion failure. A) Severe ISR in a 66-year-old woman previously treated with metallic, new-generation DES. B) The mid and proximal RCA was treated with two 3.0×28 mm Absorb BVS deployed at 14 atm. No post-dilatation was performed. C) The patient complained of angina 14 months after treatment and a moderate ISR was observed angiographically. D) Undersizing and underdeployment of the scaffold can be seen on optical coherence tomography. Intimal hyperplasia is mild-moderate. The mean diameter on the frame shown is 1.8 mm with an area of 2.55 mm2.
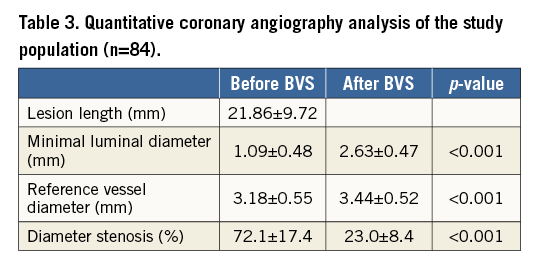
The results of the QCA analysis are shown in Table 3. Mean lesion length was 21.86±9.72 mm and the diameter stenosis reduced from 72.1±17.4% to 23.0±8.4% (p<0.001).
PERIPROCEDURAL AND IN-HOSPITAL OUTCOMES
PCI was successful in all patients and all scaffolds were delivered and deployed successfully in the target lesion. No deaths, scaffold thrombosis or repeat revascularisation occurred during the hospitalisation.
LONG-TERM OUTCOMES
Follow-up was performed in all 65 patients at six months and in 49/65 patients (75%) at 12 months (Table 4). The primary outcome, which consisted of a composite endpoint of TLR, ScT, myocardial infarction and death, was reached in 9/49 patients (18.4%) at 12 months.
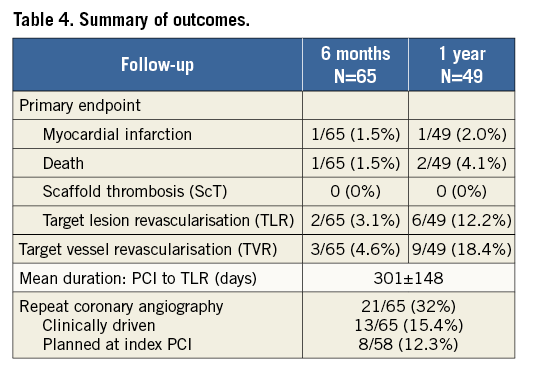
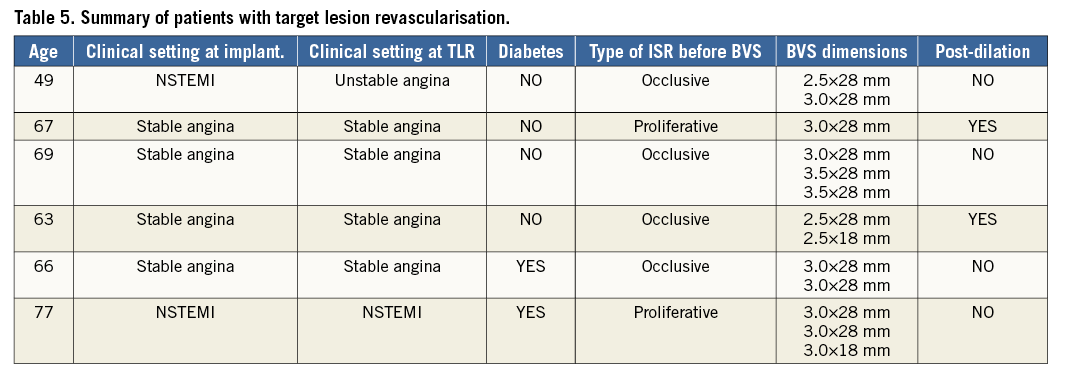
Two patients died during follow-up: one was a 75-year-old diabetic lady who presumably died due to severe pulmonary embolism seven months post-procedure. The second patient was a 68-year-old man who died of severe pulmonary fibrosis 10 months post-procedure. No scaffold thrombosis occurred during follow-up. The TLR rate was 3.1% at six months and 12.2% at 12 months. The narratives of the patients experiencing TLR are summarised in Table 5. The lesions where BVS implantation failed were either occlusive (4/6) or proliferative (2/6), and only 2/6 lesions were post-dilated. Angiographic and OCT images of a patient with TLF are shown in Figure 2.
Discussion
To the best of our knowledge, this is the first study to report outcomes in patients with ISR in metallic stents treated with Absorb BVS. Given the fact that we treated a relatively complex population with a high proportion of diabetes (26%) and with complex lesion characteristics (only 24% had focal ISR, 20% had chronic total in-stent occlusions and 21% already had two layers of metallic stents), we believe that our results are encouraging.
Although the use of new-generation DES has markedly improved PCI outcomes17, a minority of patients treated with DES will still develop ISR. These patients are difficult to treat and prone to adverse outcomes2. Current guidelines recommend DES implantation in patients with BMS or DES ISR, but the prospect of adding additional stent layers is not appealing for all patients, especially those who already have two layers of stent struts18.
The ISAR-DESIRE 3 was a randomised study comparing paclitaxel-eluting balloons (PEB) vs. paclitaxel-eluting stents (PES) vs. balloon angioplasty in patients with ISR in a limus stent19. The TLR rate at one year was 13.5% in the PES group and 22.1% in the PEB group, which indicates that the TLR rate of 12.2% in our complex population compares well to PES and might be superior to PEB.
The recently published ABSORB II randomised study demonstrated similar one-year results between patients treated with the Absorb BVS and those treated using XIENCE20, confirming that BVS can compete with well-established metallic stents. Our small pilot study takes the discussion about the daily use of BVS to the next level and indicates that even challenging lesions can be treated. Importantly, in our study all lesions were prepared using non-compliant balloons, as it is well known that underexpansion of stents is a common mechanism inducing ISR and/or stent thrombosis21-23. Underexpansion can be dramatic and is not always discernible angiographically24. Since we did not routinely use intravascular imaging to guide the procedure, we regularly performed aggressive predilatation to achieve maximal stent expansion and facilitate BVS deployment.
In the early days of BVS use (2013/early 2014), we were very cautious with post-dilatation of scaffolds, which explains why only half of the lesions were post-dilated. With increasing use of intravascular imaging (especially OCT) in our daily practice, we noticed that better scaffold expansion could be reached with post-dilatation. Additionally, on OCT imaging of patients experiencing early scaffold thrombosis, we observed that underexpansion was very frequent and thus we are currently routinely performing aggressive post-dilation of BVS using the OPN NC balloon at very high pressures (30-40 atm).
Our approach is supported by the small study of Rivero et al, in which 15 patients with ISR were treated using BVS and OCT guidance14. The authors were able to achieve good final expansion by performing high-pressure pre- and post-dilatation of the lesions. In one patient, underexpansion could not be corrected despite aggressive pre- and post-dilatation and this patient sustained subacute scaffold thrombosis.
The OPN NC is a highly non-compliant, twin-layer balloon with a rated burst pressure of 35 atm25,26. The 3.0 mm balloon only expands to 3.38 mm at 35 atm and prevents overexpansion of the 3.0 mm scaffold, which has an expansion limit of 3.5 mm.
As can be appreciated from Table 2, post-dilatation is currently being performed with high pressure (mean 27±8 atm) in order to reach maximal BVS expansion. Of note, post-dilatation was not performed in 4/6 patients with TLF and this probably resulted in underexpansion of BVS (Figure 2). Routine use of OCT to guide the procedure has the potential to improve outcomes, although this needs to be demonstrated in a prospective study.
The publication of high ScT rates in the GHOST-EU registry has raised concerns regarding the safety of the Absorb BVS27. We observed no ScT in this small population and this is reassuring.
In summary, this small, exploratory study indicates that BVS are efficient in treating ISR. The results of this registry are in line with the results of the DEB arm from the RIBS IV trial, which demonstrated a rate of freedom from TLR of 87% at one year. However, as mentioned above, the study population reported in this manuscript was more complex, including long lesions and chronic stent occlusions.
We are currently performing a prospective randomised study comparing BVS vs. DEB to treat ISR at our centre (AbsorbISR). This study includes OCT guidance of the procedure and angiographic and OCT follow-up at nine months. If our encouraging results in this retrospective study are confirmed in prospective and randomised trials, the Absorb BVS can become an alternative to DES or DEB for patients presenting with ISR.
Limitations
This was a relatively small population of patients treated with this novel approach. Although we treated a relatively complex population, selection bias might still have played a role. OCT guidance of the intervention and angiographic follow-up were available for a minority of patients. Our report must be considered a pilot project, and further studies are needed before BVS treatment for ISR can become clinical routine.
Conclusions
This study demonstrates that BVS can be safely used to treat ISR in metallic stents. Event rates are low in this small study of complex patients. The proof that BVS are a good option to treat ISR will have to be established in a prospective randomised study.
| Impact on daily practice ISR in metallic stents is not uncommon in daily practice and currently DEB or DES can be used to treat it. Both DEB and DES have their limitations and we evaluated whether BVS could be a good option to be used in this situation. The results of this study are encouraging as we demonstrate that BVS are safe to treat ISR in metallic DES. Importantly, good pre- and post-dilatation needs to be performed in order to achieve maximal scaffold expansion and full apposition. The importance of post-dilatation is highlighted in Moving images 5-7. |
Conflict of interest statement
P. Jamshidi, R. Kobza and F. Cuculi have received an institutional, unrestricted research grant from Abbott Vascular. P. Jamshidi and F. Cuculi have received lecture fees from Abbott Vascular. The other authors have no conflicts of interest to declare.
SUPPLEMENTARY DATA
The case of a 57-year-old man with ISR in the mid and distal LAD is shown. This gentleman underwent OCT-guided treatment with implantation of two Absorb BVS.
Moving image 1. Severe ISR in the mid and distal LAD.
Moving image 2. A 2.5×15 mm OPN balloon at 30 atm was used to predilate the ISR lesions. Residual stenosis is seen despite high-pressure predilatation.
Moving image 3. A 2.5×28 mm Absorb is implanted in the distal part at 12 atm and prolonged proximally with a 3.0×23 mm Absorb at 14 atm (minimal overlap).
Moving image 4. After aggressive post-dilatation with a 3.0×20 mm OPN balloon at 35 atm, a much better expansion of the scaffold can be observed.
Moving image 5. OCT recording of the distal and mid LAD is shown after predilation with a 2.5×15 mm OPN balloon at 30 atm.
Moving image 6. OCT recording of the distal LAD after the implantation of a 2.5×28 mm Absorb at 12 atm. Underexpansion can be seen.
Moving image 7. After aggressive post-dilatation with a 3.0×20 mm OPN balloon at 35 atm, a much better expansion of the scaffold can be observed.
Supplementary data
To read the full content of this article, please download the PDF.
Severe ISR in the mid and distal LAD.
A 2.5×15 mm OPN balloon at 30 atm was used to predilate the ISR lesions. Residual stenosis is seen despite highpressure predilatation.
A 2.5×28 mm Absorb is implanted in the distal part at 12 atm and prolonged proximally with a 3.0×23 mm Absorb at 14 atm (minimal overlap).
After aggressive post-dilatation with a 3.0×20 mm OPN balloon at 35 atm, a much better expansion of the scaffold can be observed.
OCT recording of the distal and mid LAD is shown after predilation with a 2.5×15 mm OPN balloon at 30 atm.
OCT recording of the distal LAD after the implantation of a 2.5×28 mm Absorb at 12 atm. Underexpansion can be seen.
After aggressive post-dilatation with a 3.0×20 mm OPN balloon at 35 atm, a much better expansion of the scaffold can be observed.