Abstract
Aims: We present here the first-in-man case report of a patient with a significant residual “intra-clip” jet treated by the implantation of an AMPLATZER Vascular Plug II.
Methods and results: A 64-year-old gentleman came to our attention for mitral regurgitation (MR) recurrence four years after transcatheter mitral repair with MitraClip. After the implantation of two further MitraClips, residual intra-clip MR was present, without room for a further clip. An AMPLATZER Vascular Plug II was successfully deployed between the two clips. Final echocardiography showed residual mild MR, without any sign of mitral stenosis.
Conclusions: This case demonstrates the feasibility of the implantation of an AMPLATZER Vascular Plug between two MitraClips to treat significant residual “intra-clip” MR, when the implantation of an adjunctive clip is not feasible. This approach may represent an effective therapeutic solution in case of a significant residual intra-clip jet.
Introduction
Percutaneous edge-to-edge mitral valve repair with the MitraClip® system (Abbott Laboratories, Abbott Park, IL, USA) has been demonstrated to have a proven safety and efficacy profile in selected patients with both functional mitral regurgitation (FMR) and degenerative mitral regurgitation (DMR)1,2. Different series have shown that more than one clip may be required in up to 50% of cases to obliterate residual regurgitation after the implantation of the first clip1,2. When medial or lateral residual MR is present, one or more adjacent clips may be positioned in order to achieve satisfactory results, especially in case of adverse valve morphology and in the presence of a broad jet3,4. However, significant residual regurgitation may persist between two adjacent clips (“intra-clip” jet). The management of residual “intra-clip” MR is a challenge and, when it occurs, it is usually left untreated.
Transcatheter closure of mitral periprosthetic leak (PVL) is a therapeutic option for high-risk patients with symptomatic PVL and may be performed through transseptal access. We present here the first-in-man case report of a patient with a significant residual “intra-clip” jet treated by the implantation of an AMPLATZER Vascular Plug II (St. Jude Medical, St. Paul, MN, USA).
A 64-year-old gentleman came to our attention for MR recurrence four years after transcatheter mitral repair with MitraClip. Transoesophageal echocardiography showed a double orifice mitral valve with severe MR (eccentric olosystolic jet, proximal isovelocity surface area [PISA] radius 10 mm), with preserved systolic function (LVEF 67%) (Figure 1, Moving image 1). The clip was not implanted perpendicular to the line of coaptation: as a consequence, the leaflet prolapse was not properly fixed and residual prolapse was still present at both sides of the clip (Figure 2, Moving image 2). The patient was admitted in NYHA functional Class II-III after an episode of decompensated heart failure in the previous month. He had a clinical history of persistent atrial fibrillation, prior percutaneous transluminal coronary angioplasty (PTCA) on the left descending coronary artery, systemic arterial hypertension and severe chronic renal failure. The EuroSCORE II estimated risk of operative mortality was 4%. After formal Heart Team discussion, agreement was reached on attempting a redo MitraClip procedure, mainly based on his frail status.
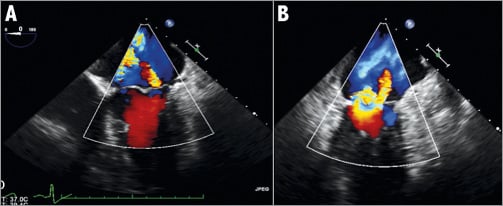
Figure 1. Pre-procedural transoesophageal echocardiography. Severe mitral regurgitation (A), with a predominant lateral regurgitant jet (B).
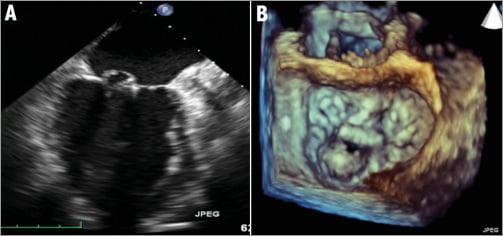
Figure 2. Intercommissural view. Residual prolapse due to the non-perpendicularity of the clip (A); 3D reconstruction confirmed the non-perpendicular position of the clip and the residual posterior leaflet prolapse on both sides of the previously implanted clip (B).
The intervention was performed under general anaesthesia and 2D and real-time 3D transoesophageal echocardiographic (TEE) and fluoroscopic guidance, as usual. A first clip was delivered through the steerable transfemoral transseptal delivery system and implanted medially to the previous one to fix the medial residual leaflet prolapse. A second clip was then implanted laterally to treat a significant residual jet and to fix the residual lateral prolapsing segment. Due to the non-perpendicularity of the previously implanted clip with respect to the coaptation line, it was not possible to fix completely the residual lateral prolapse with the second clip, which was properly implanted. Therefore, moderate to severe residual MR was still present between the two lateral clips (“intra-clip” jet), due to a residual prolapsing spot (Figure 3, Moving image 3). However, there was no room for a further clip to treat residual MR. Therefore, we decided to attempt the obliteration of the residual regurgitant jet by the implantation of a vascular plug between the two clips, similar to a perivalvular mitral prosthetic leak closure via the transseptal approach. After the removal of the clip delivery system, an AMPLATZER 7 Fr sheath (St. Jude Medical) was advanced in the left atrium through the steerable guidance catheter, in the proximity of the origin of the residual jet. A Terumo Straight wire (Terumo Corp., Tokyo, Japan) was used to cross the “intra-clip” jet and then exchanged for an Amplatz Super Stiff™ wire (Boston Scientific, Natick, MA, USA). An AMPLATZER Vascular Plug II 18 mm was delivered and then deployed between the two clips (Figure 4, Moving image 4). Final echocardiography showed mild residual MR (Figure 5, Moving image 5), without any sign of mitral stenosis. Finally, femoral venous access was secured with a “figure of eight” cutaneous suture. No complication occurred during the procedure. The patient was discharged uneventfully five days after the intervention under double antiplatelet therapy (acetylsalicylic acid 100 mg/die and clopidogrel 75 mg/die).
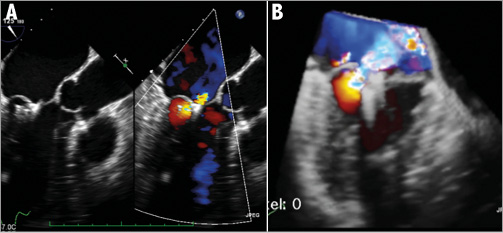
Figure 3. Residual significant “intra-clip” regurgitant jet between the two more lateral clips. LVOT view (A) and 3D reconstruction view (B).
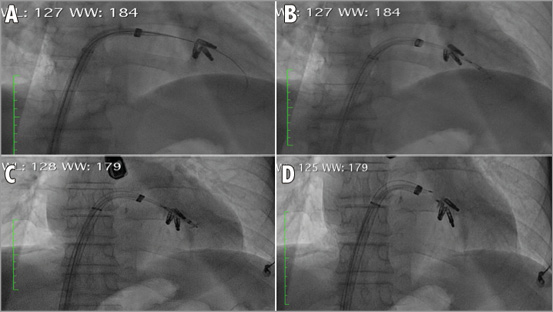
Figure 4. Positioning of the AMPLATZER Vascular Plug. Advancement of the Terumo wire in the left ventricle through the “intra-clip” jet (A); advancement of the device with the opening of the distal disc in the ventricle (B); pull-back of the plug (C); opening of the proximal disc in the left atrium and final detachment (D).
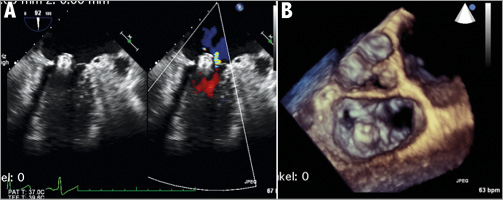
Figure 5. Final results. Residual mild mitral regurgitation (A) and final aspect in the 3D echo surgical view (B).
This case demonstrates the feasibility of the implantation of an AMPLATZER Vascular Plug between two MitraClips to treat significant residual “intra-clip” MR, when the implantation of an adjunctive clip is not feasible. In this case, this approach was associated with an important reduction of the residual MR, suggesting that this therapeutic option may be effective and could be considered in selected cases. Although long-term follow-up is warranted to appraise the durability of this combined procedure, this approach may represent an effective therapeutic solution in case of significant residual intra-clip jet.
| Impact on daily practice The management of residual “intra-MitraClip” mitral regurgitation is a challenge and, when it occurs, is usually left untreated. The approach here described was associated with an important reduction of residual intra-clip MR, suggesting that this therapeutic option may be an effective solution in selected cases for an unsolved clinical problem. |
Conflict of interest statement
F. Maisano is consultant for Abbott Vascular. The other authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Pre-procedural transoesophageal echocardiography showing severe mitral regurgitation (A), with residual posterior leaflet prolapse and a predominant lateral regurgitant jet (B).
Moving image 2. X-plane view showing the residual prolapse due to the non-perpendicularity of the clip (A); 3D reconstruction confirmed the non-perpendicular position of the clip and the residual posterior leaflet prolapse on both sides of the previously implanted clip (B).
Moving image 3. Significant residual “intra-clip” regurgitant jet in the LVOT view (A) and in the 3D reconstruction view (B).
Moving image 4. Positioning of the AMPLATZER Vascular Plug: advancement of the Terumo wire in the left ventricle through the “intra-clip” jet (A); advancement of the device and the opening of the distal disc in the ventricle (B); pull-back of the plug (C); opening of the proximal disc in the left atrium and final detachment (D).
Moving image 5. Final results showing mild residual mitral regurgitation (A) and final aspect in the 3D echo surgical view (B).