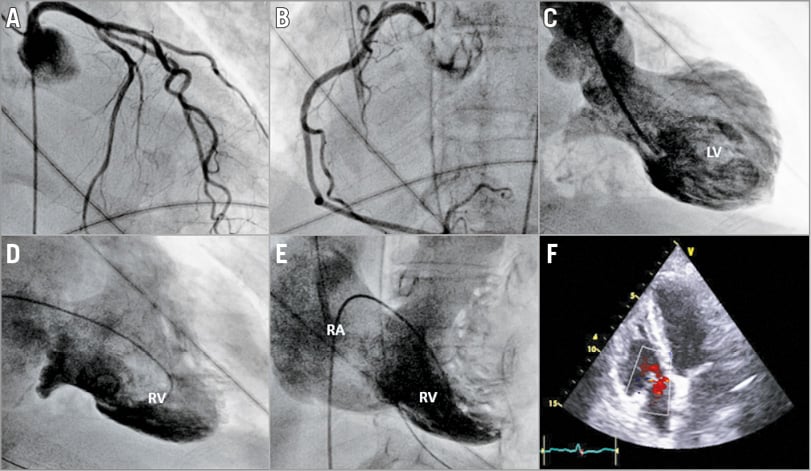
An 80-year-old woman was admitted to our department for orthopnoea. Three days before, she had undergone emergent colostomy for acute sigmoiditis. At physical examination, she presented with pulmonary crepitations and jugular venous distension. Baseline ECG showed sinus rhythm with T-wave inversion in the precordial leads. Laboratory test results demonstrated moderate troponin I elevation with a peak level of 5.16 µg/l. Emergent coronary angiography was performed and showed the absence of obstructive coronary disease or angiographic evidence of plaque rupture (Panel A, Panel B). Left ventricular (LV) angiography disclosed akinesia and ballooning of the mid-apical LV segments with sparing of the base (Panel C, Moving image 1). Left ventricular ejection fraction (LVEF) was estimated to be 30%. Contrast right ventriculography also demonstrated apical ballooning of the right ventricle (RV) with hyperkinesia of basal segments (Panel D, Moving image 2). In addition, end-systole RV angiography revealed severe tricuspid regurgitation with right atrial (RA) opacification as intense as the RV (Panel E, Moving image 3). At three-day follow-up, transthoracic echography (TTE) confirmed the diagnosis of biventricular Takotsubo cardiomyopathy (TTC) showing complete recovery of LV and RV wall motion abnormalities. Furthermore, TTE revealed complete disappearance of tricuspid regurgitation (Panel F, Moving image 4).
TTC in its classic pattern (LV apical ballooning) is sometimes associated with mitral regurgitation when the hyperdynamic state of the basal segments results in obstruction of the LV outflow tract. In the case of biventricular TTC, right ventricular dysfunction may also precipitate transient severe tricuspid regurgitation, the mechanism of which remains to be elucidated.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Left ventriculography (RAO 30° view) showing ballooning of the mid-apical LV segments.
Moving image 2. Right ventricular angiography (RAO 30° view) showing apical ballooning of the right ventricle.
Moving image 3. Right ventricular angiography (LAO 30° view) revealing acute severe tricuspid regurgitation.
Moving image 4. Transthoracic echography (apical 4-chamber view) showing recovery of wall motion abnormalities and disappearance of tricuspid regurgitation.
Supplementary data
To read the full content of this article, please download the PDF.
Left ventriculography (RAO 30° view) showing ballooning of the mid-apical LV segments.
Right ventricular angiography (RAO 30° view) showing apical ballooning of the right ventricle.
Right ventricular angiography (LAO 30° view) revealing acute severe tricuspid regurgitation.
Transthoracic echography (apical 4-chamber view) showing recovery of wall motion abnormalities and disappearance of tricuspid regurgitation.