Background
The current success rates of percutaneous coronary interventions (PCI) of chronic total occlusions (CTO) are estimated to be above 90% by experienced CTO operators. The retrograde approach has contributed significantly to this increase. Wire externalisation represents the important final step within the retrograde approach. This expert review article aims to illustrate and explain the different kinds of techniques of wire externalisation as well as important tips and tricks. Crucial steps and bail-out techniques of wire externalisation during retrograde PCI of CTOs are summarised. Further information is given on how to avoid possible complications. This expert review addresses both the beginner and the experienced CTO operator.
INDICATIONS
Wire externalisation in retrograde PCI of CTOs means advancing the retrograde guidewire into and through the antegrade guiding catheter to serve as an antegrade route for balloon and stents.
DIFFICULTIES
Several parameters have to be taken into account prior to retrograde wiring: the length of the intracoronary loop depending on the length and tortuosity of the anatomic course of the collateral connection (CC), the diameter of the left ventricle and, last but not least, the patient’s size. Therefore, before starting the procedure, we recommend using shorter 90 cm guiding catheters, at least for the donor artery, and long retrograde (≥150 cm) microcatheters (MC) to start with for all retrograde CTO attempts in which wire externalisation is planned. As in all retrograde procedures, it is important to measure the activated clotting time (>350 sec) every 30 mins during the procedure.
Methods
Before starting the externalisation, the retrograde dedicated CTO wire first has to cross the occlusion and re-enter the correct lumen with the support of an MC positioned 2-3 cm proximal to the wire tip. Then the retrograde CTO wire may be advanced and fed into the antegrade guiding catheter (Figure 1A, Figure 1B).
Now the MC is advanced further over the conventional guidewire 2-5 cm into the antegrade guiding catheter (Figure 1C). If the MC cannot be advanced into the guide because of a hard occlusion, tortuosity or friction, an antegrade trapping balloon (2.5-3.0 mm) should be placed into the distal guide and inflated at about 8 atm to trap and fix the retrograde wire. This will increase support and allows advancing the MC into the antegrade guide.
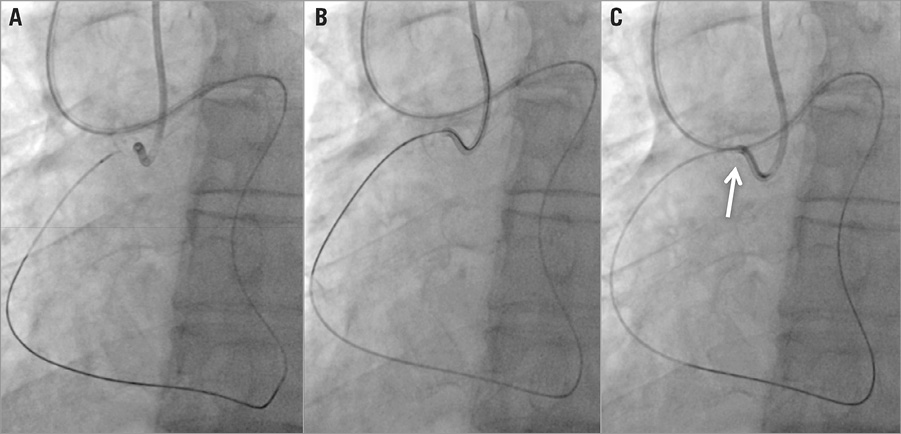
Figure 1. Conventional wire externalisation. A retrograde MC is advanced towards the antegrade cap of the proximal CTO of the RCA (A). The retrograde guidewire engages the antegrade guiding catheter (B). The retrograde MC engages the antegrade guiding catheter (white arrow) (C). After retracting the retrograde guidewire the externalisation wire is advanced retrogradely via the externalisation route within the retrograde MC towards the antegrade guiding catheter (not shown).
Now the retrograde CTO wire is pulled and replaced by the externalisation wire via retrograde MC into the antegrade guiding catheter, finally exiting at the antegrade haemostatic valve.
Conclusions
Wire externalisation represents the important final step in the retrograde approach. Our review is addressed to both the beginner and the experienced CTO operator. The extended online version of our review outlines in more detail all the important issues dealing with the externalisation process and gives a stepwise description of wire externalisation in retrograde CTO PCI.
Conflict of interest statement
The authors have no conflicts of interest to declare.