Abstract
Aims: To evaluate the angiographic and clinical outcome of patients undergoing paclitaxel-eluting stent (PES) implantation for unprotected left main coronary artery (ULMCA) stenosis in a multicentre, prospective registry. The overall event rate for PCI of ULMCA disease remains higher than in on-label use making additional outcome data and risk-stratification tools for the ULMCA population desirable.
Methods and results: A prospective registry included all patients with a significant (>50%) stenosis in ULMCA disease. In 151 of these patients the target lesion involved the distal bifurcation in 100 patients (66%), which was treated by predominantly using a “provisional T stenting” strategy.
In distal ULMCA disease group, 72% had only one stent implantation while 28% had multiple (either 2 or 3) stents implanted. At a median follow-up of 472±75 days, cardiac death occurred in 3 patients (2%) and major adverse cardiac and cerebrovascular events (MACCE) in 16 patients (10.6%).
Conclusions: In the drug-eluting stent era, paclitaxel eluting stent implantation of ULMCA stenosis provided excellent immediate and mid-term results in this selected population, suggesting that it may be considered as a safe and effective alternative to CABG for selected patients with ULMCA who are treated in institutions performing large numbers of PCI procedures.
Abbreviations and acronyms
BMS: bare metal stent
CABG: coronary artery bypass graft
CAD: coronary artery disease
DES: drug eluting stent
DLMD: distal left main disease
FRIEND: French multicentre registry for stenting of unprotected LMCA stenosis
IVUS: intravascular ultrasound
LAD: left anterior descending artery
LCX: left circumflex artery
LMCA: left main coronary artery
MACE: major adverse cardiac event
MACCE: major adverse cardiac and cerebrovascular event
MI: myocardial infarction
MLD: mimimal luminal diameter
MSCT: multislice computer tomography
PES: paclitaxel eluting stent
PCI: percutaneous coronary intervention
PTCA: percutaneous transluminal coronary angioplasty
QCA: quantitative coronary angiography
RCA: right coronary artery
RVD: reference vessel diameter
SES: sirolimus eluting stent
STEMI: ST elevation myocardial infarction
TIMI: thrombolysis in myocardial infarction
TLR: target lesion revascularisation
TVR: target vessel revascularisation
ULMCA: unprotected left main coronary artery
Introduction
Left main coronary artery (LMCA) disease has remained a challenge for percutaneous coronary intervention (PCI) throughout the last 25 years. In the bare metal stent (BMS) era, early results were very promising, but the long-term results showed too many restenotic events for PCI to compete with coronary artery bypass graft (CABG). The marked decrease in restenosis rates observed with drug-eluting stents has prompted explorations of their use in unprotected left-main coronary artery (ULMCA) disease. Preliminary data, mainly retrospective and single centre studies, suggest that sirolimus-eluting stents (SES) and paclitaxel-eluting stents (PES) implantation are each associated with better six-months results than bare-metal stents in ULMCA disease1-4 although target-vessel revascularisation (TVR) rates remain somewhat higher in many series for distal left main bifurcation lesions, particularly when multiple stent techniques (T, Kissing, or crush) are used5,6. By and large, however, the effectiveness of DES in ULMCA has still not been good enough to replace CABG in LMCA revascularisation of patients who are good surgical candidates. The aim of the present study was to evaluate the angiographic outcome of ULMCA stenosis percutaneous intervention using the TAXUS Express-2 PES Stent System (Boston Scientific, Natick, MA, USA) in a prospective multicentre registry.
Methods
Patient selection and study population
FRIEND – the French multicentre RegIstry for stEnting of uNprotecteD LMCA Stenosis – included 23 clinical centres and a coordinating centre. The participating hospitals were selected on the basis of recognised experience with PCI of unprotected LMCA stenoses. To be eligible for the registry, patients had to have angiographic evidence of >50% diameter stenosis of the LMCA suitable for stent placement, with either anginal symptoms or documented myocardial ischaemia. Exclusion criteria consisted of contraindications to antiplatelet or anticoagulation therapy, emergency situations such as acute ST-elevation myocardial infarction (STEMI) or cardiogenic shock, serum creatinine > 1.8 mg/dl, reference vessel diameter < 2.5 mm or > 4.5 mm, in-lesion restenosis, severe obstructive pulmonary disease, pregnancy women, and life expectancy less than three years to underlying medical conditions. Between December 2005 and July 2006, a total of 600 patients with ULMCA disease were screened; 445 patients (74%) did not comply with the clinical or angiographic requirements for inclusion, or refused to give informed consent. Of these, 45.4% had CABG treatment, 36% PCI treatment. For the remaining patients (18.7%) the coronary features were unsuitable for CABG or PCI and were treated by medical therapy. One hundred and fifty-five consecutive patients (26%), who underwent PES placement in an unprotected LMCA stenosis, were enrolled in the prospective registry (Figure 1).
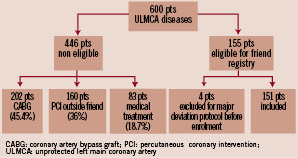
Figure 1. Selection of study population.
Angioplasty procedure
PCI technique, including the selection of arterial access or predilation devices, IIbIIIa inhibitors, prophylactic intra-aortic balloon pump use, and intravascular ultrasound (IVUS) guidance, was left to the discretion of the operator. However, the use of a “provisional T stenting” strategy was strongly recommended in the treatment of distal left main lesions, in which a single PES was implanted from left main, preferentially through the left anterior descending artery (LAD). A second stent was implanted in proximal circumflex only if there was a residual moderate to severe dissection or significant residual stenosis after final kissing-balloon inflation. All elective patients were pretreated with aspirin and clopidogrel beginning at least 3 days before angioplasty. Unfractionated heparin, 50-70 U/kg (with a goal activated clotting time of >250 s), or bivalirudin, was administered during the procedure. All patients were instructed to take daily aspirin 160 mg indefinitely and clopidogrel 75 mg for at least 12 months. Cardiac enzymes were determined routinely after percutaneous coronary procedures, at 8 hour intervals during the first 24 hours, or until discharge. At least one post-procedural 12-lead electrocardiogram was obtained and compared with pre-intervention tracings.
Angiographic methods
Quantitative coronary angiography was performed by an off-site, independent core laboratory (Corisis system) using a validated edge-detection program. The projection showing the maximal degree of stenosis was selected at baseline and was used for systematic angiographic control. For purposes of bifurcation analysis, the LMCA of each patient was divided into the parent vessel and side branch. By convention, the parent vessel was defined as the LMCA and proximal LAD, and the side branch as the LCX. The target lesion was defined as involving the distal LMCA if it was within 3 mm of the circumflex ostium. For the parent vessel and side branch, the reference vessel diameter (RVD), minimal luminal diameter (MLD), acute luminal gain (MLD immediately after the procedure minus the MLD before the procedure), binary restenosis (diameter stenosis of >50% relative to the angiographically uninvolved left main lumen), percent diameter stenosis, and late luminal loss (MLD immediately after the procedure minus the MLD at follow-up) were measured separately. In-stent restenosis was defined angiographic restenosis anywhere inside or within 5 mm of the stented segment.
Endpoints and definitions
The primary endpoint was the occurrence of in-stent restenosis at 9-months follow-up. The secondary endpoints were the rate of major adverse cardiac and cerebrovascular events (MACCE) at one, 12, 18 and 36 months. The LMCA was defined as “unprotected” if there was no history of CABG. Non-Q-wave myocardial infarction (MI) was defined as creatine kinase greater than two times the upper limit of normal with an abnormal CK-MB in the absence of pathological Q waves. Stent thrombosis was defined as any of the following angiographic demonstration of stent closure or intrastent filling defect, unexplained sudden death, or MI without concomitant documentation of a patent stent. Acute stent thrombosis was defined as thrombosis occurring within 24 hours, subacute thrombosis between 24 hours and 30 days, and late thrombosis more than 30 days after the index procedure. Target lesion revascularisation (TLR) was defined as any repeat intervention (surgical or percutaneous) to treat a stenosis anywhere within the LMCA or within 10 mm distal to the LAD and LCX ostia. Target lesion revascularisation was further characterised as “ischaemia-driven” if signs or symptoms of ischaemia were present. MACCE were defined as any MI, any TLR, thrombosis, stroke, or death. Technical success was defined as a final diameter stenosis <30% and Thrombolysis in Myocardial Infarction (TIMI) flow grade 3.
The European system for cardiac operative risk evaluation (EuroSCORE) which is based on patient, cardiac and operation related factors, was used to stratify the risk of death at 30 days7,8. According to this scoring system, the patients were stratified as risk patients if the logistic EuroSCORE was >6 (see http://www.euroscore.org/calc.html).
Data collection and follow-up
The study protocol was approved by the FRIEND Review Board, the French Society of Cardiology, and was conducted in accordance with the Declaration of Helsinki. All patients signed informed consents before elective procedures, and data were reported using a standard case report form, and then forwarded to the coordinating centre. Clinical information about death, myocardial infarction, repeated revascularisation, bypass surgery, and stroke was obtained during clinic visits or telephone interviews and was evaluated by a Clinical Event Committee which was independent of the operators. All the patients were followed up for at least 36 months.
Statistical analysis
The size of the cohort of patients was based on being able to show a 50% relative reduction in in-stent restenosis compared to the literature rate of 30% for BMS9-12, with alpha and beta errors of 5% (i.e., p < 0.05) and 20% (i.e. 80% power), respectively. One hundred and thirty-one patients were required. With the estimated attrition due to death, or lost for angiographic follow-up, the total number of inclusion was a maximum of 150 patients. Categorical variables were expressed as counts and percentages and continuous variables as mean±SD. Angiographic characteristics and coronary angiography measurements were presented according to distal or non-distal ULMCA disease. Results were compared using Student’s t-test for continuous variables, Chi-square test or Fisher’s exact test for categorical variables. Logistic regression analyses were used to determine risk factors influencing 9-month in-stent restenosis and MACCE rates. The considered covariates were: age, diabetes mellitus, EuroSCORE, vessel reference diameter, distal ULMCA disease, baseline angulation between LAD and LCx (< or >70°), use of single vs multiple stents and final post PCI MLD .
Cumulative probability of survival free from cardiac death, total death and MACCE were drawn for the whole population, and for distal versus non-distal ULMCA disease as sub-groups. Survival free from MACCE was also drawn in distal LMCA disease for patients with one stent versus 2-3 stents in distal left main lesion. All p values were 2-tailed, with statistical significance set at a level of < 0.05. Confidence intervals were calculated at the 95% level. All analyses were performed using SAS software version 8.2 (SAS Institute Inc, Cary, NC, USA).
Results
Baseline characteristics
Concerning intention to treat, 155 patients were enrolled in this trial. However, four patients were excluded at the beginning of enrolment for major protocol deviation (one death before coronary stenting, one acute coronary syndrome < 12 hours, one patient with a contra-indication to antiplatelet therapy and one PCI involving only balloon angioplasty). Thus, 151 patients were included in this prospective registry after percutaneous intervention of the ULMCA using one or more PES.
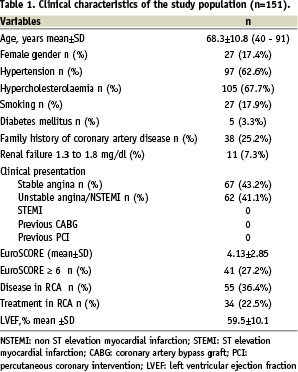
Clinical, procedural and angiographic characteristics are summarised respectively in Tables 1, 2 and 3. The procedure was elective for stable angina or silent ischaemia in 89 patients (59%), with no emergency revascularisation procedures for ST-elevation myocardial infarction or cardiogenic shock. Diabetes mellitus was only present in five patients (3.3%) and renal failure in 11 patients (7.3%), but 55 patients (36.4%) had additional disease in the RCA, 34 of which were treated during the index procedure. Twenty-seven percent of patients had an estimated EuroSCORE operative mortality > 5%.
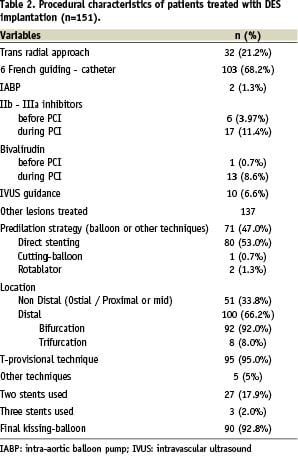
One-hundred (66%) patients had distal LMCA stenosis: 92 were bifurcations and 8 were trifurcations. For this group, T-provisional technique was performed in 95% of cases, with 72% of patients receiving only 1-stent, and 28% receiving 2 or 3 stents. Final kissing-balloon dilation was performed in 93% of case, and 20 patients (13%) received glycoprotein IIb/IIIa inhibitors before or during the procedure. Technical success was achieved in all patients.
In-hospital and long-term MACCE
In-hospital and 12-month clinical outcome are illustrated in Table 4. Three patients (2%) with high-risk EuroSCORE died of acute stent thrombosis during hospitalisation. One patient underwent TLR for residual dissection of LCx outside the previously stented segment. The combined endpoint of MACCE including death, stroke, any MI, TLR, or thrombosis thus occurred in six patients (4%), before hospital discharge. MACCE between hospital discharge and 12-month follow-up occurred in another 10 patients, so the cumulative incidence MACCE occurred in 16 patients (8%) by 12-months. Kaplan-Meier MACCE free of survival is shown in Figure 2. There was no significant difference in clinical outcome between patients with vs. without distal left main disease, although there was a non-significant statistical trend towards lower MACCE in non-distal (i.e., proximal or mid) lesions as shown in Figure 3 (hazard ratio [HR] 0.82, 95% confidence interval [CI] 0.27 to 2.51; p=0.73). For distal lesions, the MACCE rate through 12-month follow-up remained slightly lower for patients receiving a single stent versus multiple
(2 or 3) stents, but this difference did not reach statistical significant differences (HR 1.09, 95% CI 0.29 to 4.1; p=0.89). (Figure 4)
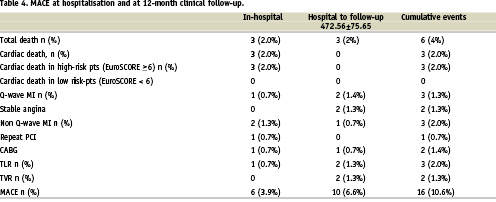
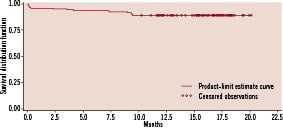
Figure 2. Actuarial rate of event free survival.
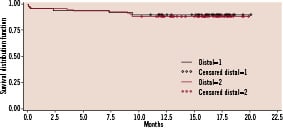
Figure 3. Actuarial rate of event free survival between non-distal and distal left main disease.
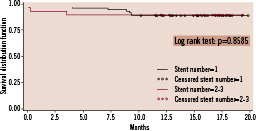
Figure 4. Actuarial rate of event free survival between one and two or three stents implantation in distal left main disease.
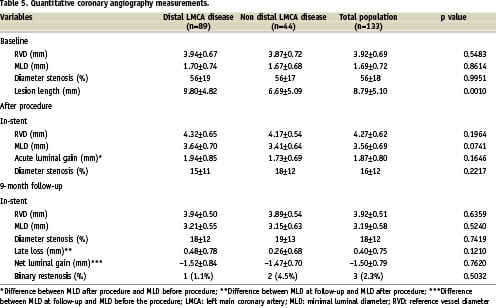
Quantitative coronary angiography
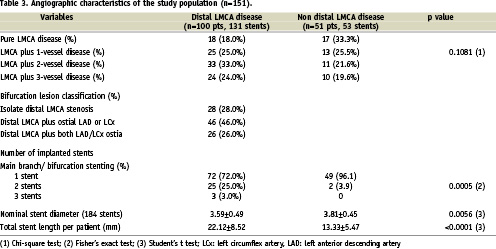
Overall, follow-up angiography was performed in 133 patients. Angiography was not performed in 18 patients because of death before the scheduled angiography (4 patients), patient refusal (8 patients), age > 80 or serious comorbidities (6 patients) and the absence of clinical symptoms of cardiac ischaemia. Baseline and follow-up angiographic results are shown in Table 5. As shown, despite a similar LMCA reference vessel diameter, patients with distal lesion location tended to have a longer lesion length and a slightly greater MLD. In-stent acute luminal gain was similar in both groups, but late loss in the distal ULMCA disease was almost double that of proximal or mid-lesions (0.48±0.78 mm vs. 0.26±0.68 mm, p=0.12). Binary restenosis occurred only in three of the 133 patients studied (2.3%), including two (4.5%) of 44 patients with ostial or mid-shaft LMCA stenosis and in one (1.1%) of 89 patients with bifurcation involvement.
Discussion
The percutaneous treatment of LMCA disease has remained a challenging task, with historically unacceptably high long-term adverse event rates9-12. However, the outcomes associated with percutaneous coronary intervention have improved dramatically with the introduction of stents, high-pressure balloon dilation, and glycoprotein IIb/IIIa inhibitors13.
Procedural safety
Many studies of unprotected LMCA PCI have been published. Most have involved the Cypher sirolimus-eluting stent (Cordis, Miami Lakes, FL, USA) or both SES and PES1-6,14. The largest such series to date includes 220 patients, and the smallest only 50 patients. Procedural success (diameter stenosis < 30% in the absence of MACE) was high (90-100%) in each series, with a low rate of in-hospital death (0.8-2.0%). All studies had low (2.3-3.1%) use of debulking devices prior to stent placement, compared with the higher rates of debulking used in the pre-DES era. The present study is similar to these other DES series of ULMCA in showing a favourable (2%), 30-day mortality after stenting of unprotected LMCA stenosis in elective teatment, supporting consideration of this therapy as an alternative to bypass surgery in selected patients.
Nine month angiographic and 12-month clinical outcome
The advent of BMS offered only slight improvement in the percutaneous treatment of unprotected left main lesions15,16 due to the continued frequent occurrence of in-stent restenosis (some of which was fatal in presentation)9,10. Recently, the liberal use of DES to treat LMCA has been shown to favourably affect restenosis compared to that with BMS2-4, but the rate of major cardiovascular events still remains high in the first series of patients in the DES era3,4. Several studies have shown better medium-term prognosis when unprotected LMCA stenting is confined to low-risk groups (i.e., excluding acute myocardial infarction, poor left ventricular function, or cardiogenic shock), with good clinical stability through six months after revascularisation15,16. In the current study of a similarly restricted population, the primary endpoint of angiographic in-stent restenosis rate at 9-months was only 2.3% and was statistically significantly lower than the benchmark comparison of 30% in-stent restenosis rate for BMS. This was associated with
a low incidence of clinical events through 12-months. These results in the future could change our practice with maybe a systematic control of ULMCA stenting not by QCA but by MSCT.
These extremely favourable short- and long-term outcomes in the current study, with no major events during the follow-up period have several potential explanations. First, this population as opposed to other trials11,17, had a low percentage (3.3%) of diabetic patients, good left ventricular ejection fraction, good renal function, mean age of 68.3±10.8 years, and a large reference vessel diameter of 3.92±0.69 mm. Second, this prospective multicentre registry of 23 participating centres is the first to systematically study the provisional T-stenting approach for distal left main disease (DLMD) rather than the double stent techniques used in many prior studies. The earlier literature has consistently shown significantly worse long-term outcomes in patients undergoing percutaneous treatment of distal compared to proximal or mid-vessel LMCA lesions. Valgimigli et al5 showed that distal LMCA disease carried independent negative prognostic implications that should be considered when selecting the most appropriate patients for LMCA intervention. With our use of provisional T stenting (and mostly (72%) single stent technique and final kissing-balloon in 93%), however, the procedural success and short-term (30 days) outcome was remarkably similar between proximal mid and distal lesions. Although there was still a weak trend towards slightly higher rate of events at 12-month follow-up, driven mainly by a higher rate of TVR in the DLMD group, the avoidance of more complex multi-stent techniques such as crush, V, culotte or kissing stenting in the current series may well account for our excellent mid-term results. We cannot, however, prove this benefit here given the small number of such multiple stent patients in our series. At the same time, DES implantation in non-bifurcation left main coronary artery lesions showed an excellent (0.9%) long-term restenosis rate, with a favourable (7.4%) rate of any major adverse clinical event, compared to prior studies19. Unlike the left main Taxus pilot study18, we didn’t find any impact of bifurcation angle between LAD and LCx (< or > 70°) at 12-month clinical outcome. In our registry, even luminal late loss is greater in DLMD than in non DLMD (0.48±0.78 mm vs 0.26±0.68 mm), there is no difference and no predictive factors in terms of in-stent restenosis.
PCI with DES vs CABG
Even though current guidelines still recommend surgical revascularisation for LMCA stenosis, it is clear that the PCI approach using DES offer an increasingly excellent alternative in selected patients. Some retrospective studies evaluating surgical treatment for left main stenosis have reported higher in-hospital mortality (1.7% to 7.0%) and 1-year mortality (6% to 14%) than seen in our study, although these surgical series were not limited to the lower risk settings studied here20,21. Three other non-randomised trials22-24 comparing CABG vs PCI, however, similarly failed to detect any difference in either mortality or the combined occurrence of MACE and major adverse cerebrovascular events at the one or two year outcomes. But none of the studies thus far has compared the safety and efficiency of DES to that of CABG in patients with LMCA stenosis in an appropriately sized randomised trial. Such randomised studies comparing CABG vs DES are now in progress, including PRE-COMBAT (Premiere of Randomised Comparison of Bypass Surgery versus Angioplasty using Sirolimus-Eluting stent in Patients with left main coronary artery disease), FREEDOM (Future revascularisation evaluation in patients with Diabetes mellitus: optimal management of multivessel disease) and SYNTAX (Synergy between percutaneous coronary intervention with Taxus and cardiac surgery study), which recently (April 2007) completed enrolment of 1,800 randomised left main and 3 vessel disease patients including 710 patients with left main disease. These studies, will hopefully more closely evaluate the benefits of DES in the treatment of selected patients with LMCA disease.
Study limitations
First, our findings in carefully selected patients may not be able to be generalised to the entire range of unprotected LMCA stenosis. Second, the data does not necessarily apply to interventional cardiologists with less prior experience with LMCA stenting. Third, the results of our study are very encouraging, but they cannot be conclusive until the conclusion of pending studies with larger sample sizes and more prolonged clinical follow-up; all of which is clearly needed to confirm our findings and extend our capability to risk-stratify this challenging subset of patients24,25.
Conclusions
The event rate after percutaneous treatment of ULMCA disease in the FRIEND multicentre registry seems to be remarkably low, with an excellent short and long-term prognosis in a low surgical risk population. Our current findings extend the previous knowledge about risk stratification and technical approach and may be helpful in identifying the most appropriate LMCA patients in whom catheter-based intervention perhaps offers the best alternative to bypass surgery. Additional data from large scale randomised trials like SYNTAX, will be forthcoming to shed further light on this important subgroup of patients.
Acknowledgement
The authors thank all investigators and research coordinators who contributed to the successful completion of this study, as well as Donald S. Baim who kindly provided editorial assistance. We are indebted to Drs. Michel Bertrand, Victor Legrand and Jean-Jacques Goy for their support in conducting the clinical events committee providing editorial assistance and to the French Society of Cardiology who were the responsible body for the management of this study.
