While large randomised trials have failed to demonstrate a clinical benefit from routine aspiration thrombectomy1, innovative strategies are needed, particularly in patients with a large thrombus burden.
We report the case of a 57-year-old male presenting with inferior ST-segment elevation myocardial infarction. Patient consent was obtained for the publication of this article. Coronary angiography revealed a heavily thrombotic occlusion of the right coronary artery. Even after guidewire crossing and predilation, the thrombus persisted with sluggish distal flow. Mechanical aspiration (CAT RX [Penumbra, Inc.]) ultimately restored Thrombolysis in Myocardial Infarction 3 flow with ST-segment resolution and chest pain relief, although a large distal thrombus remained. Stenting was therefore deferred, and intensive antithrombotic therapy was initiated with dual antiplatelet therapy (DAPT; aspirin and ticagrelor) plus glycoprotein IIb/IIIa inhibitors (tirofiban), followed by unfractionated heparin infusion until repeat angiography.
At three-day follow-up, angiography still showed a large, organised thrombus (Moving image 1). Since aspiration alone had failed in the acute phase, a combined strategy utilising a stent retriever (SR; enVast 4.5x46 mm [Vesalio]) and aspiration was adopted.
Two guidewires (SION blue [Asahi Intecc]) were advanced into the distal right coronary artery through a Judkins right 4 (JR4) 7 Fr guiding catheter: one for SR delivery and the other as a safety wire to maintain distal access. A microcatheter (Rebar [Medtronic]; inner diameter 0.021") was advanced over one guidewire (Figure 1A, Moving image 2), then removed, allowing for SR advancement (Figure 1B, Moving image 3). The SR was positioned across the thrombus, and the microcatheter was withdrawn to capture it (Figure 1C, Moving image 4). To minimise embolic risk during SR removal, a 7 Fr guide extension catheter (Telescope [Medtronic]) was advanced proximally to the SR (Figure 1D, Moving image 5) with the CAT RX aspiration system directly connected to the Y-valve on the JR4 guiding catheter (Supplementary Figure 1). The SR was then withdrawn into the guide extension catheter (Figure 1E, Moving image 6), and subsequently into the JR4, under continuous aspiration. The final angiogram showed complete thrombus clearance (Moving image 7, Supplementary Figure 2); this was confirmed by optical coherence tomography, which revealed intraplaque haemorrhage without rupture (Moving image 8). In this context, stenting was avoided. The patient had an uneventful recovery and was discharged on DAPT.
Although SR-assisted thrombectomy is well established in neurointervention, either with syringe-based aspiration (SAVE technique)2 or continuous aspiration (SOLUMBRA technique)3, evidence remains scarce in the coronary field.
Recent reports have demonstrated the feasibility and safety of negative-pressure syringes combined with various mechanical thrombectomy systems45. Our case represents the first coronary application coupling an SR with continuous aspiration using the CAT RX system. This synergistic strategy enhances efficacy, where aspiration alone had previously failed. Sustained negative pressure with an SR and guide extension catheter may further reduce embolic risk, albeit at a higher cost. To date, no strategy has demonstrated clear clinical superiority, and larger studies are warranted.
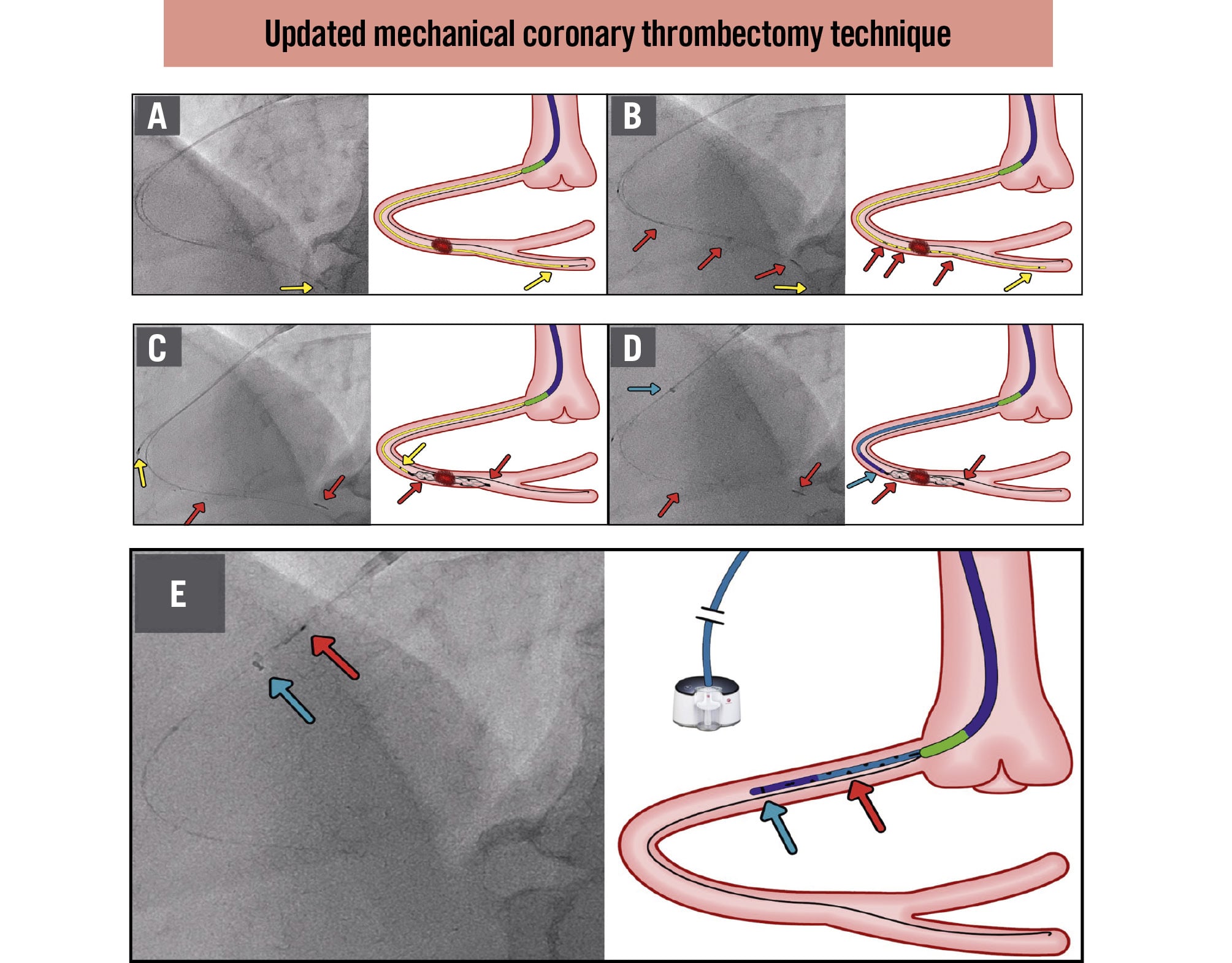
Figure 1. Updated mechanical coronary thrombectomy technique. A) Microcatheter (yellow arrow) advanced over the guidewire. B) SR (red arrows) advanced through the microcatheter after guidewire removal. C) Microcatheter withdrawn, allowing SR delivery across the thrombus. D) Guide extension catheter (blue arrow) advanced proximally to the SR (while aspiration is connected). E) SR retrieved into the guide extension catheter and then into the JR4 under continuous aspiration with the CAT RX system. JR: Judkins right; SR: stent retriever
Conflict of interest statement
J.F. Iglesias reports speaker fees honoraria from Penumbra, Inc. M. Roffi received institutional research grants from Cordis, Terumo, Boston Scientific, Biotronik, and Vascular Medical. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Large persistent thrombus at repeat angiography.
Moving image 2. Microcatheter advanced over the guidewire.
Moving image 3. SR advanced through the microcatheter after guidewire removal.
Moving image 4. SR positioned across the thrombus.
Moving image 5. Guide extension catheter advanced proximally to the SR.
Moving image 6. SR retrieved into the guide extension catheter.
Moving image 7. Final angiogram showing complete thrombus removal.
Moving image 8. OCT showing minimal residual thrombus with intraplaque haemorrhage without rupture.