Continuing Medical Education (CME) is a specific form of postgraduate education whose aim is to help healthcare professionals (HCPs) to consolidate their competences and upgrade their knowledge. In conventional CME, faculty members develop and deliver programmes. They define what, and how, learners need to learn.
This established system is at odds with the current media environment. HCPs are information seekers navigating the continuous flow of information from the internet, journals, digital tools and meetings. Because HCPs increasingly need to self-direct their own learning, they are more likely to experience disorienting dilemmas, cognitive conflicts and confusion.
This established system is also at odds with evidence in adult learning theory (ALT). “Andragogy” – the art and science of helping adults learn – has explored how adult education develops critical skills (problem-based learning), applies knowledge to workplace situations (situated learning), and builds interpersonal skills (cooperative learning).
Transformative learning forms part of ALT. “Transformative learning integrates questioning and revising how learners develop expectations based on their reflections on experience and knowledge”. Learners are made aware of their specific needs to reach new levels of proficiency. In short, the learning process may become transformative when it is self-initiated and based on a self-reflection on knowledge and prior experience, rather than on the interpretation or judgement of “authority figures”.
The next sections expand on the ways in which transformative learning theory (TLT) has advanced the threefold research agenda of ALT (problem-based, situated and cooperative learning), including in the field of medical education.
Problem-based learning: transformation based on critical learning
Problem-based learning seeks to sharpen adults’ critical skills rather than to increase their knowledge. Problem-based learning is itself problematic. For instance, scholars debate whether learners are more likely to remember and implement positive, or negative, results. TLT goes beyond this conundrum. It considers that HCPs should not only learn or critique techniques, but also reconsider assumptions upon which their practice is based. In other words, TLT is a critical framework that should have a lasting impact on HCPs, regardless of existing consensus or controversy. To develop critical skills, however, learning should not tackle any problem, but HCPs’ problems.
Situated learning: transformation based on professional experience
“Situated learning” portends that knowledge is meaningful if it is applicable to working situations. In other words, adult educators should comprehensively take into account learners’ daily needs through in-depth practice assessment rather than solely relying on literature reviews or faculty input. TLT shares this approach: its starting point is to revisit HCPs’ practice when it becomes problematic – either because it leads to unexpected outcomes or because its relevance is questioned under new circumstances. TLT therefore presents HCPs with the opportunity to solve problems that they face in the workplace. To solve these problems and revise assumptions, TLT recommends acting within a group.
Cooperative learning: transformation based on small group learning
Both ALT and TLT credit groups for being learning engines. Studies in postgraduate medical education have demonstrated the added value of interactive teaching in general, and group learning in particular, to improve medical care. Groups prompt peer pressure, accountability and critical reflection, socialisation and group identification. TLT argues that dialogue within groups helps the learners to “stand out of themselves” to answer their problems and revise their assumptions. Moreover, identifying with a group may enhance learning and, ultimately, create a community of learners united in a shared experience.
In short, the new media environment and evidence-based ALT show that a new educational paradigm is required - one that is built around the active involvement of participants who become actors of their learning. This learner-centric approach first requires undertaking an in-depth practice assessment to identify HCPs’ experience and their desired learning outcomes. It also compels course organisers to provide HCPs with a safe learning environment in which they can critically reflect upon available data and share and learn from one another. In short, TLT implies moving from a classic lecture-discussion format towards the concept of a “community of learners” engaged in “collaborative critical learning”.
To the authors’ knowledge, there is scant reported experience on the alternative educative method of transformative learning (TL) in the framework of large postgraduate courses in interventional cardiology. LabCom RiMeC (ReInventing the MEdia Congress) is a joint research programme between the LLA-CREATIS research lab (University of Toulouse Jean Jaurès) and Europa Group, a company specialising in the organisation of medical congresses. LabCom RiMeC is financed in particular by the National Agency for Research and the Region of Occitanie. This ambitious research programme strives to create new forms of knowledge transfer within medical congresses. It takes stock of the transformation of the media environment and the impact this may have on the purpose and promise of vocational training. It builds on theory, analytical tools and innovation drivers in the fields of the arts and media (intermediality and applied theatre) in particular, and social sciences and the humanities more broadly, drawing on research in the arts and media to rethink medical congresses. LabCom RiMeC conducted a quasi-experimental study of a specific TL module entitled “At the heart of the problem: let’s self-direct a learning trajectory and content”. With this module, course organisers aimed at providing evidence to further the development of needs-driven educational and professional development activities. The module integrated:
– a process to identify the individual targeted learners’ learning gaps and learning expectations;
– the implementation of TL theory during EuroPCR 2016 (the programme of EuroPCR 2016 is available at https://www.pcronline.com/Courses/EuroPCR/EuroPCR-2016).
Methodology
The aims of this experiment were:
1. to assess the feasibility of a tailored learning trajectory answering the expectations of all participants, and enabling them to build and deliver during EuroPCR 2016 a collective learning content based on collaborative critical thinking;
2. to evaluate the short-term and long-term impact of the learning trajectory on practitioners’ confidence in various professional competences (critical thinking, clinical performance and communication skills), and on the creation of a “community of learners” within a group of early-career interventional cardiologists.
Based on ALT in general, and TLT in particular, we formulated the following hypotheses.
HYPOTHESES
PROBLEM-BASED LEARNING
Transformative learning enhances learning outcomes because it develops participants’ critical skills, regardless of whether results presented during the educational intervention are consensus-based or not.
SITUATED LEARNING
Transformative learning enhances learning outcomes because it comprehensively takes into account participants’ learning needs.
COOPERATIVE LEARNING
Transformative learning enhances learning outcomes because participants co-construct a learning content within groups and deliver it to an audience.
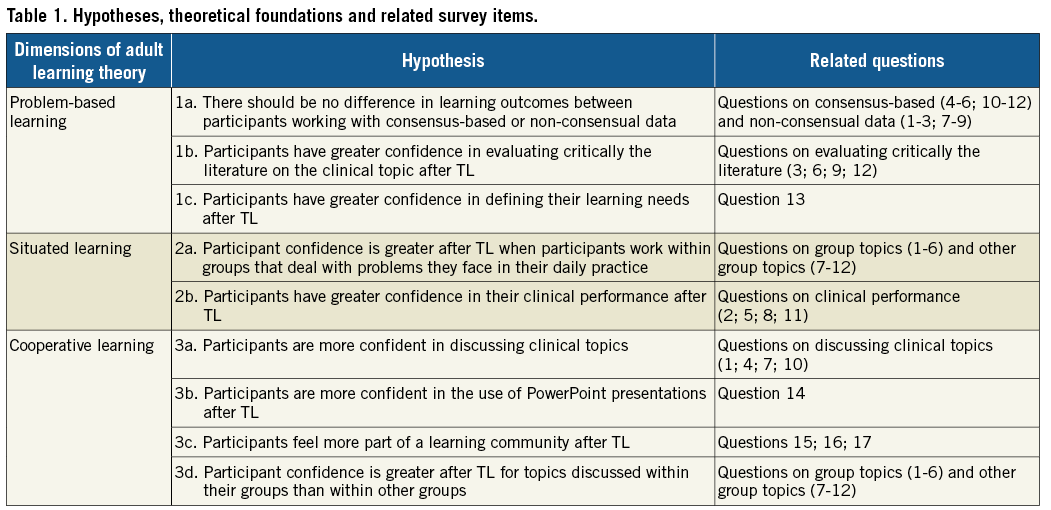
Table 1 sums up the operationalised hypotheses as well as the corresponding theoretical foundations and survey items.
PARTICIPANTS’ RECRUITMENT
We used purposive sampling to recruit participants in order to ensure the representation of different countries and practices. After using lists of the European Association of Percutaneous Cardiovascular Interventions and screening participants’ cover letters, 18 early-career interventional cardiologists were included in the study.
INDIVIDUAL IN-DEPTH PRACTICE ASSESSMENT
In the module, TL was blended with flipped learning. Flipped learning is a process by which students direct their learning trajectory and construct their own training paths with the help of a mentor before the physical meeting.
Before EuroPCR 2016, three rounds of individual email exchanges between one mentor and participants took place. Their aim was to explore participants’ daily practice and personal questions, problems, cognitive conflicts or disorienting dilemmas. Participants reported gaps in their knowledge and professional performance and learning expectations.
ON-SITE ENABLING ACTIVITIES – INSTRUCTIONAL METHODOLOGIES
During EuroPCR 2016, meetings with mentors were organised. On the first day, participants were allocated to five small groups focusing on various interventional cardiology topics. The five topics were techniques (fractional flow reserve [FFR], optical coherence tomography [OCT], etc.), complex percutaneous coronary intervention (PCI) and chronic total occlusion (CTO), stents, percutaneous valve treatment and left atrial appendage closure (LAAC), and STEMI/NSTEMI. Participants were then introduced to a common method to collect and critically analyse information found in the extant literature and EuroPCR 2016 sessions, and to tools and techniques to prepare and present public lectures. During the remainder of EuroPCR 2016, each group’s members attended sessions and explored other available resources. On the last conference day, groups delivered a presentation of their findings to their peers.
DATA COLLECTION AND ANALYSIS
This study used a qualitative approach to obtain an in-depth understanding of participants’ perception of the module. In the short term, we evaluated participants’ satisfaction throughout the learning trajectory with logbooks, a satisfaction questionnaire and participant observation.
In the long term, we assessed TL impact on practitioner confidence 20 months after the module. We used a retrospective pre-test to post-test survey to measure changes in practitioner confidence before and after the self-directed learning trajectory. This theory-driven questionnaire was based on existing competences established by regulators, as well as on a literature review of psychometric surveys for health educational interventions dealing with HCPs’ confidence in specific clinical knowledge, skill or attitude, communication and feedback skills, and self-directed/life-long learning. We adapted Tian to measure practitioner declarative confidence (or perceived behavioural control).
Based on group topics and presentations, we asked each participant three series of questions. The first series explored clinical items discussed within the participant’s own group (consensus-based and non-consensual data). The second series dealt with clinical items presented by other groups. For the first and second series, consensus-based and non-consensual data were discussed along three dimensions: a) discussing the issue with a colleague, b) recommending the clinical behaviour to a patient, and c) critically evaluating the literature related to the issue. The third series of questions assessed HCPs’ confidence in their communication skills and their sense of belonging to a “community of learners”.
Results
Out of 18 participants, 13 completed the logbooks, 17 responded to the satisfaction questionnaire, and 13 participated in the interviews conducted 20 months after EuroPCR 2016.
OVERALL RESULTS
Overall, participants were satisfied with the TL experience. Seventeen (17) out of 18 participants expressed the view that the collective learning content was clear and satisfied their needs. This satisfaction appears to translate into practitioner confidence after TL. Indeed, overall practitioner confidence increased by two points (on a range from one to seven) before and after TL (Figure 1).
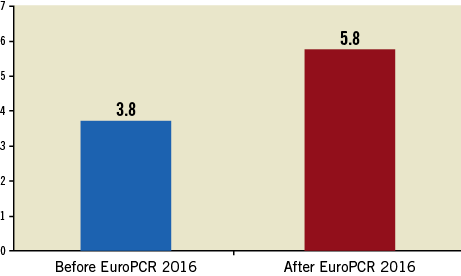
Figure 1. Average confidence discussing, using and evaluating certain clinical practice before and after EuroPCR 2016 (from 1=very little to 7=very much).
THE BENEFITS OF SELF-DIRECTED CRITICAL LEARNING
In accordance with the benefits of problem-based learning, TL organisers developed participants’ critical awareness in formulating their learning needs. On average, participants’ confidence in defining their learning needs after TL increased by 2.4 points (from 3.8 out of seven to 6.2 out of seven) (Figure 2). This lends support to hypothesis 1c (TL increases the confidence in defining one’s learning needs).
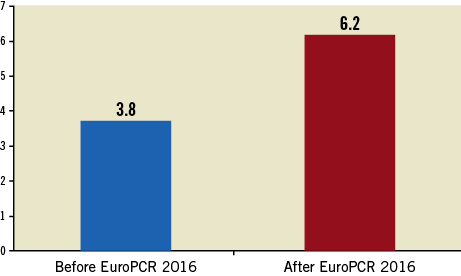
Figure 2. Average confidence defining learning needs before and after EuroPCR 2016 (from 1=very little to 7=very much).
DISCUSSING AND CRITICISING RATHER THAN CHANGING CLINICAL PRACTICE
Our data confirmed that participants gained more confidence in their critical abilities than in modifying their practice. During EuroPCR 2016, only 3 out of 13 participants considered that they attended TL to find answers in their daily practice. Conversely, all participants reported being able to share their critical viewpoints effectively during the module. Therefore, TL appears to offer HCPs a forum to reflect critically on available data rather than to address their daily practice.
Our interviews also show that participants had the lowest confidence when discussing and evaluating data on clinical topics before TL, and that this is where they progressed the most (an increase on average of two points in both cases). Moreover, TL participants’ confidence in preparing and presenting lectures also grew (on average +2.2 points on a 1-7 range). These findings tend to confirm hypotheses 1b (confidence in evaluating the literature) and 3a (confidence in discussing clinical topics).
In short, what participants sought in TL was to share and confront their experience rather than to revamp their clinical practice.
DEVELOPING GENERIC CRITICAL THINKING RATHER THAN SOLVING SPECIFIC ISSUES
Paramount in TL is the development of learners’ critical skills rather than the provision of definite answers to existing consensus or controversies. Our interviews corroborate this view and its related hypothesis 1a: we observed no significant difference in confidence changes when participants discussed consensus-based (+2 points) and non-consensual (+1.8 points) data. Indeed, TL participants discussing non-consensual data – the use of FFR in emergency or of haemodynamic support in STEMI patients – also displayed greater confidence after TL in not performing certain procedures. As an interviewee explained when discussing a controversial medical practice, “I am really confident for not using it”.
One example of critical awareness stood out during EuroPCR 2016. Participants in group 3 discussed the superiority of bioresorbable drug-eluting stents over permanent metallic drug-eluting stents. They concluded that “to date we don’t have “solid” information demonstrating the clinical benefits of bioresorbable drug-eluting stents over permanent drug-eluting stents in our patients with complex lesions”. What was a dissenting view then became mainstream as specific bioresorbable stents were taken off the market in late 2017.
THE BENEFITS OF GROUP WORK: A COMMUNITY OF LEARNERS
During our experiment, participants were allocated to groups dealing with problems they faced in their daily practice, but groups also provided learners with platforms to discuss topics with other participants. Did participants feel more confident after EuroPCR 2016 engaging with topics discussed within their group, rather than those discussed in other groups? Our observations invalidate hypotheses 2a and 3d: we did not observe any significant impact of group belonging on practitioner confidence. The average change of confidence for one’s group topics was +2.1 points, and was +1.7 points for topics discussed in other groups.
Though more evidence should be collected to understand group dynamics, we venture some possible explanations for this finding.
One reason for this insignificant difference could be that participants were not allocated to the group that discussed problems relevant to their practice. However, we can confidently rule out group allocation problems as the explanation. First, only one out of 18 participants considered in 2016 that topics selected in his group were remote from his learning needs. Second, participants overall declared having less confidence before TL for clinical topics that were discussed in their own group. In short, they worked on topics of their own interest and of which they usually considered they had the greatest knowledge and practice gaps.
Another reason could be that, irrespective of group topics, participants did not work very well together within groups. This could have had a negative impact on their confidence after TL. However, as previously mentioned, all participants felt that the group had given them the opportunity to convey their views, which rules out the claim that negative group dynamics hindered the collective learning process.
We argue that belonging to the broader TL session was more important than belonging to a specific group. Participants learnt from all groups, not only their own. Several indicators point to the creation of a community of learners through TL. First, we observed contamination across groups throughout the training module. For instance, all groups followed the lead of group 4 in using the PICOT method to analyse published studies. Second, participants considered that TL at EuroPCR 2016 developed their sense of identification with the “PCR community”. At EuroPCR 2016, 9/10 respondents declared feeling part of a PCR community. Twenty months later, the most significant change they reported was also “feeling part of the PCR community”. This more than doubled, from 2.3 to 5.6 points (on a 1-7 range). Moreover, 11 out of 13 TL participants remain in touch with their peers, whether through informal or professional networks (Figure 3).
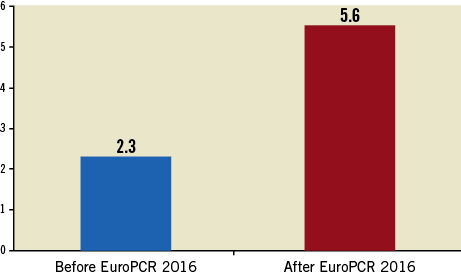
Figure 3. Overall feeling part of the PCR community, before and after EuroPCR 2016 (from 1=very little to 7=very much).
When disaggregating the “feeling part of the PCR community”, we observed that no participant was impervious to the benefits of TL. On the one hand, participants who continued to be involved in PCR events strongly identified with the PCR community. One interviewee indicated:
“We were given the sense that this was a useful project. Not only that, but also the follow-up and the involvement in other things enabled there to be some continuation, that this was not only one event in time.” (interviewee no. 5)
Conversely, participants not invited to engage in other PCR meetings, expressed their disappointment:
“I was never contacted or integrated into EuroPCR for anything, and I will participate this year only because I sent my research to contribute to the congress, and not vice versa. Honestly, I have to admit that probably I expected more impact of that participation into the programme.” (interviewee no. 8)
In short, there is untapped potential in TL modules to further participants’ sense of belonging within the medical community.
Discussion
OUR RESULTS IN THE LIGHT OF EVIDENCE-BASED ADULT LEARNING
Overall, self-directed TL seems to stimulate problem-based and cooperative learning rather than situated learning. On the one hand, practitioners did not attend TL to change their practice, nor did they change their practice significantly after their EuroPCR 2016 experience. This supports the idea that practitioners attend conferences and seminars to consolidate their practice rather than to change it. On the other hand, in line with TL theory, we observed that TL participants learnt first and foremost how to sharpen their critical thinking, whether to define better their learning needs or to appraise existing tools, techniques and data in the field of interventional cardiology.
Similarly, TL extended cooperative learning across all groups. Feeling part of a PCR community then was dependent on whether participants were included in subsequent PCR activities. The positive and negative impact of TL on participants’ feelings supports the claim that TL course organisers should not overlook participants’ emotions.
In any case, this experience’s positive outcomes on practitioners’ confidence in solving problems and working as a group lend further support to the TLT.
ORIGINAL CONTRIBUTION OF OUR RESEARCH
This module also innovated in the field of TLT because we combined TL with flipped learning. Participants not only participated in TL activities during EuroPCR 2016, but also provided upstream work prior to the conference to define their learning needs better. Course organisers considered that participants required guidance not to find information, but to find relevant information within the flow of available data. It is possible that learning how to use this critical framework also distinguishes these young cardiologists as a community of learners:
“We all have been taught in medicine, but using that framework allows to place the information where it needs to be, and that is for any topic. (…) In learning the framework for critical analysis, this has led me to teach other people about this framework, and also to learn myself about that kind of teaching. I’ve used it with junior doctors, nursing students, and even colleagues.” (interviewee no. 5)
Though we can draw numerous benefits from this educational experience, our study displays methodological limitations as well as caveats in the design of the TL module itself.
Caveats and limitations
RESEARCH DESIGN
First, the small sample used in this contribution precludes statistically significant relationships, a caveat we have compensated for with participant observation and qualitative interviews. Nonetheless, the use of a retrospective survey may have introduced a number of biases (halo effect and recall bias), in addition to using self-reported data. In future experiments, one could mitigate these issues by planning data collection better.
Second, this quasi-experimental design does not account for covariation. While we establish temporal precedence, we cannot know whether better TL leads to better performance. This observational study, or formative evaluation, is a promising start to understanding the mechanisms of self-directed critical group learning and improving it. It may be the basis for hypotheses then to be tested in a comparative and controlled study design.
Third, though we used and adapted a questionnaire whose validity and reliability had been tested, we did not test our adapted questionnaire against measures of validity and reliability as methodologically required.
MODULE DESIGN
Though course organisers used flipped learning to identify participants’ needs, the choice of topics discussed during TL could still be improved. Some participants were very seldom confronted with cases requiring a practice discussed during TL, while others mentioned that some specific devices were not available in their workplace.
Additionally, the TL module was by and large disconnected from the rest of the EuroPCR 2016 conference. Tellingly, TL participants at EuroPCR 2016 indicated that about one third of resources made available during the conference were not useful. Instead, they made use of other available (online) resources in the broader media environment.
Last but not least, the TL experience had mixed effects on the creation of a community of learners. It had a positive impact on participants engaged in additional activities, but a negative impact on others.
Conclusion
Experimenting with TL at EuroPCR 2016 suggests that the combination of TL and flipped learning consolidates participants’ confidence in their critical thinking. It may also further the sense of community within the field of interventional cardiology. Future research should examine if and how “transformative learning” initiates “communities of learners” beyond educational interventions, as well as how group dynamics within TL lead to more or less practitioner confidence. Last but not least, further research should look into if and how other congresses have included such innovative learning and evaluated it.
Mainstreaming flipped learning and TL into broader medical conferences is required. EuroPCR conferences offer such an opportunity thanks to the EuroPCR fellowship programme for young practitioners, in which flipped learning could be introduced to tailor the programme to participants’ needs better. Additionally, it is not enough to include practitioners in a single educational experience. It is necessary, in order to avoid negative outcomes in a broader community, to fulfil one’s commitments by engaging practitioners in additional activities. More fundamentally, while the medical world now advances in line with evidence-based medical findings, so should the medical community, and CME organisers, move forward in using evidence-based adult learning to design more effective outcomes-based CME.
Acknowledgements
The research was conducted thanks to grants from the National Agency for Research, the Region of Occitanie and the Europa Group.
Conflict of interest statement
The authors have no conflicts of interest to declare.
The complete list of references can be found in the online version of this paper.
To read the full content of this article, please download the PDF.