Coronary revascularisation in the Asia Pacific region
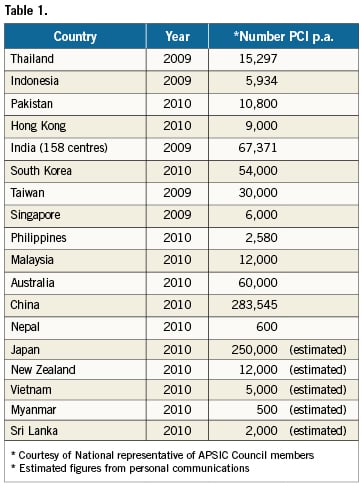
There is great heterogeneity in the development of percutaneous coronary intervention (PCI) in the Asia Pacific region. Japan and Australia were among the first countries to begin PCI services in 1981. The latest reported number of PCIs performed annually in the Asia Pacific countries is illustrated in Table 1.
Differences in coronary revascularisation between the East and the West
Coronary revascularisation by coronary artery bypass graft (CABG) surgery was well advanced in many developed western nations well before the advent of percutaneous transluminal coronary angioplasty (PTCA) in 1977. In contrast, CABG is still not available in most hospitals providing PCI therapy in the Asia Pacific countries. The ratio of PCI to CABG in Asia can be as high as 20:1 as compared to 3:1 in the West. The reasons for this are complex. Lack of CABG expertise and facilities, socio-economic, cultural, philosophical and religious preferences as well as the relative ease to start PCI services are among the key factors. Aided by the rapid economic progress in many Asian nations, PCI centres mushroomed in many hospitals in Asia Pacific countries over the past decade, notably China.
PCI practice differences between the East and the West
The lack of surgical facilities in many hospitals providing PCI services in the Asia Pacific countries means that there is no choice but to use PCI to treat all patients needing revascularisation therapy, despite their high lesion complexities and clinical risks. This is a vicious cycle that has hampered the development of CABG in many Asian hospitals. The practice of PCI in the Asia Pacific countries therefore, cannot follow western PCI guidelines, such as those of the ACC/AHA and ESC. Many Asian countries have developed local practice guidelines that are slightly different to those of the West.
In addition to practice guideline differences, data from pivotal clinical trials such as SYNTAX cannot be applied to patients in Asia Pacific countries. For example, the mortality and MACE rates of CABG especially cannot be achieved in many hospitals in the East. Therefore, the recommendation of PCI or CABG for Asian patients cannot be based solely on western clinical trials. Furthermore, the cost of therapy can often influence the choice of therapy modality against standard western practice guideline recommendations in the Asia Pacific region. For example, CABG is cheaper than PCI in India because of the high cost of stents and other devices. Cheaper, locally produced stents and drugs are used clinically in Asian countries, notably India and China, often without clinical trials to test their efficacy or safety.
PCI training considerations in the Asia Pacific region
Relatively few Asian fellows have the privilege to learn PCI in overseas western centres of excellence. Most learn their skills from local proctorships and courses, as well as the pre-eminent western PCI courses such as the EuroPCR and TCT. These western live demonstration courses have played a significant role in the development of PCI in the Asia Pacific region. In the past decade a healthy collaboration between the East and the West has evolved, resulting in hybrid East-West live courses such as TCT-Asia Pacific, SingLive-EuroPCR, CIT-TCT, CCT-AP and many others. The generous and selfless transfer of knowledge and skills from the more advanced western operators during these live courses as well as e-learning programs are crucial to the rapid growth of PCI in the Asia Pacific region. For the aspiring young Asian PCI operators, “live-demo” courses must emphasise more the “why” and not only the “how” of PCI to optimise patient outcome. The principle that patients who agreed to participate in live demonstration courses are there to be treated rather than just used for teaching must be observed by trainers at all times.
Availability of PCI to Asia Pacific patients
A “good and useful” therapeutic modality for a common disease must be available to all who need it. If the cost of a therapy is restricted to only those who could afford it, it is relatively useless. PCI is such a therapy for coronary patients in the developing countries in the Asia Pacific region. Manufacturers of devices and adjunctive drugs necessary for PCI therapies must balance the cost and profit margins of their life saving products and make PCI available to as many as possible patients who need them before it can be a really good and useful therapy.
Resolving differences between East and West
There will always be two different worlds, the “haves” versus the “have-nots” eastern values versus those of the West. These two worlds can be likened to two pyramids, one upright with a broad base at the bottom (“bottom-up”) which represents the West, and the other, with the broad base at the top (“top-down”) representing the East. If the two pyramids were to overlap, it will produce a star, with a common hexagonal area in the middle and six protruding horns. Applying this to the practice of PCI, or any endeavour for that matter, in the East and the West, one should work synergistically in the common hexagonal area to bring PCI forward in to the future. The protruding “horns” representing differences between the two worlds should be left alone. PCI workers in the East can absorb the labour of research, educational activities and the clinical scrutiny of the West. In turn the West can capitalise on the unique operative skills accumulated through shear necessity to treat the large number of patients. Finally, the global multinational medical and device companies should try to make their life-saving products accessible to all those who need them. With these synergies, PCI will definitely continue to thrive and help patients in the East and West alike.
