Abstract
Aims: There is no data about the utilisation of a single guiding catheter for current routine, transradial, right and left coronary diagnosis and intervention. We investigated the feasibility and safety of using 6Fr, Ikari left (IL) 3.5 guiding catheter for this purpose.
Methods and results: This prospective single-centre study enrolled 621 consecutive patients referred for transradial coronary angiography with ad hoc coronary intervention. The radial artery was successfully accessed in 96.8% of patients. Right and left coronaries were successfully engaged in 98.1% of cases. Engagement with good back-up at right and left coronaries (device success) was achieved in 96.6% of cases. Coronary intervention was performed in 61.2% of the cases, among them, 84.5% had coronary stenting. Procedure success was 98.2%. Procedure time was 21.4±15.1 and 65.4±36.1 minutes; mean fluoroscopy time was 6.8±7.2 and 24.1±18.9 minutes and mean contrast volume was 96.2±45.3 and 197.9±46.2 ml for diagnostic and interventional cases respectively. One patient (0.16%) had catheter related radial artery spasm and three patients (0.48%) encountered a catheter induced RCA dissection.
Conclusions: Right and left coronary angiography and intervention is feasible and highly successful using IL 3.5 as a single transradial guiding catheter.
Introduction
Cardiac catheterisation by transradial artery access has shown a low rate of vascular complications1, earlier ambulation2, lesser cost and better patient’s comfort3. However, the radial artery is a small and spastic artery4. Its tortuosity and some variant anatomy5,6 make the radial access and transradial catheterisation more technically demanding, with a steeper learning curve7,8. Various kinds of guiding catheters have been designed to comply with lesser manipulations using the transradial approach9,10.
Using a single guiding catheter for transradial left and right coronary diagnostic and percutaneous coronary intervention (PCI) procedures is an attractive idea, with potentially less procedure and fluoroscopy time, lower costs, and diminished radial artery spasm. A prior limited experience, in selected cases, had been reported, almost ten years ago, using a single guiding catheter (Kimny radial, Schneider Co. Minnesota, USA) for transradial PCI9. However, there is no data about utilisation of a single guiding catheter for all comers, routine, right and left coronary diagnosis and intervention with the currently available PCI devices.
The Ikari curve-guiding catheter (Terumo, Tokyo, Japan) has two different design sets for the right and left coronaries10. Herein we present our single centre experience using 6Fr Ikari left (IL) 3.5 guiding catheter for right and left coronary diagnosis and intervention, as a prospective practical experience.
Materials and methods
Design, patients and approach
This prospective, single-centre cohort study enrolled 621 consecutive patients referred for coronary angiography with ad hoc PCI, when indicated, through the radial artery access. The exclusion criteria were uraemia and the general contra-indications for cardiac catheterisation11. For the first two hundred cases, all cases were performed by four operators (the authors), using IL 3.5 guiding catheter, including 30% of cases performed by a beginner with one-year experience of transradial intervention (TRI), for the following cases, additional junior trans-radialists learned and used the catheter. Left radial access was the default access for the operators, unless left radial pulse is impalpable. Using a biplane catheterisation machine, six views were routinely taken for the left coronary artery (LCA) and four views for the right coronary artery (RCA), followed, when indicated, by left ventriculography and or aortography with a 6Fr pigtail catheter. The process of balloon predilatation, stenting, or adopting alternative intervention devices were left to the discretion of every operator. All patients have given a written consent prior to the procedure, and the centre’s Committee on Human Research approved the protocol.
Device description
The left and right Ikari catheters for coronary catheterisation were thoroughly described before10,12,13. Ikari left guiding catheter basically has a similar shape to the Judkins left (JL) catheter except for the area of the brachial-cephalic angle12. Judkins catheters designed for trans-femoral interventions (TFI) are inappropriate to fit the brachial-cephalic angle, when used by right radial approach, and Ikari catheter overcomes this point by a reverse angle (Figure 1).

Figure 1. Similarities between the Ikari left (IL) 3.5 guiding catheter and the Judkins left (JL) 3.5 guiding catheter, (a) IL has an additional curve on the shaft to accommodate the brachial-cephalic angle in the transradial approach. (b) Similarity comes closer when the distal segments of IL and JL catheters are placed in parallel. Note the longer third segment in IL that helps for better guiding support.
The IL catheter is available in three sizes, designated IL 3.5, IL 4.0 and IL 4.5 corresponding to the same sizes as Judkins catheters. For all IL catheters the first distal line is 0.8 cm; the second straight line is 1.1 cm for IL 3.5. The length is 1.1 cm at the third straight line and 5.9 cm at the fourth straight line for all IL catheters11.
Catheterisation technique
After local anaesthesia with 2 ml of 2% xylocaine, the radial artery was punctured with a 20 gauge, 2.5 cm long 1-piece metal (Cook®) needle and a 0.025” straight guidewire was inserted through it. Upon removal of the needle, a 16-cm long 6Fr Radifocus® introducer II sheath (Terumo, Tokyo, Japan) was advanced over the guidewire. To reduce spasm and discomfort, a drug “cocktail” containing 200 µg of nitroglycerine, and 2.5 of verapamil (unless the patient had bradycardia or heart failure) and 5000 IU of heparin were administered through the sheath side arm. The IL 3.5 catheter was advanced over a 260 cm long, J-tipped, 0.035-inch teflon guidewire (Argon Medical Devices, the Netherlands) to the ascending aorta. Either coronary artery engagement can be attempted, generally, using the same technique as the Judkins catheters.
To engage the left coronary artery in cases with dilated ascending aortic root, the catheter may need further pushing down to the aortic cusp, where the catheter tip usually engages the left main with its tip facing the left main roof. Slow pull-back usually gets the catheter in a better position co-axially with the left main coronary artery (Figure 2).

Figure 2. A case with dilated aortic root, (a) A low setting position was needed to reach and engage the left main (LM) orifice; the catheter tip is facing the LM roof. (b) Gradual pull-back is needed for better co-axial orientation, also confirmed by a gentle contrast test. (c) A clear image was finally obtained.
In a more dilated ascending aorta, additional length of the catheter can be gained by straightening the secondary curve with the teflon guidewire.
For RCA engagement; while in 60 degrees left anterior oblique projection, after certain disengagement from the left main, the catheter is turned clockwise while continuing to push its tip down near the aortic valve, until the catheter directly, and passively, engages the RCA ostium. For more horizontal and low take-off RCA, the catheter may need to be lifted up to get its tip oriented more horizontally for proper RCA engagement. In some cases, we needed to keep the teflon guidewire within the catheter, with 1-2 cm of the guidewire protruding outside. In this way the primary curve of the catheter becomes rectified, so that the IL 3.5 curve resembles a Judkins right (JR) curve (Figure 3).

Figure. 3. Close similarity between Ikari left (IL) 3.5 and Judkins right curve when IL 3.5 catheter is rectified using a teflon 0.035-inch wire.
The assembly should be turned clockwise while the guidewire is gradually pulled back until the catheter tip start facing the RCA ostium, the guidewire is then further withdrawn inside the catheter until proper catheter engagement (Figure 4).
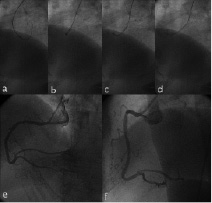
Figure 4. Engaging the right coronary artery (RCA) aided by the teflon wire in IL 3.5 catheter. The catheter with the teflon wire is rotated clock-wise (a-b), and gradually pulling-back the wire when the catheter faces the RCA orifice (c-d). The catheter engaged the RCA with both a good orientation and good angiogram obtained (e-f).
Due to the nature of the preformed IL primary curve, it might super-select the conus branch, this usually causes pressure damping, and can be confirmed by a gentle puff of a contrast test if needed. In this situation, partial catheter withdrawal may be enough. Alternatively, we disengage and re-orient the catheter tip more horizontally, or facing-down, assisted by the teflon guidewire if needed. Confirmation of coaxial catheter position before RCA angiography, in two perpendicular projections, almost completely eliminates the possibility of RCA dissection. Once engaged the corresponding coronary artery (Figure 5), the IL 3.5 often provides good back-up without further manipulation.
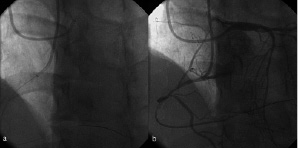
Figure 5. A case with RCA chronic total occlusion, (a) right and left coronaries engaged transradially with two Ikari left 3.5 catheters; the curve mimicked Judkins right at the RCA and Judkins left at the LM. (b) Contralateral angiogram in the left anterior oblique with cranial angulation view after successful RCA antegrade wiring (See online data supplement).
Study endpoints and definitions
The primary endpoint of this study is device efficacy (success) and safety. Device (IL 3.5 guiding catheter) efficacy was defined as successful work with stable engagement and efficient guiding support for both left and right coronary arteries, without causing catheter related complications (safety endpoint). The secondary endpoints of this study are procedural success, engagement rate, procedure time, fluoroscopy time and contrast volume used. Procedural success is defined as a minimum stenosis diameter reduction to < 50% after balloon angioplasty and < 20% after stenting, without major clinical complications (e.g., death, MI, emergency coronary artery bypass surgery) during hospitalisation14,15. Procedure time starts after successful sheath insertion, and ends by withdrawal of last catheter. Engagement time is the elapsed time from the moment the radial artery pressure was recorded through the sheath to the moment the first acceptable coronary artery angiogram was obtained. Engagement rate is the rate of successful engagement in coronary ostium with the initially-selected, IL 3.5 guiding catheter.
Crossover from radial to brachial or femoral with Ikari left 3.5 as the guiding catheter, and use of alternative guiding catheters after IL 3.5 failure is included in the final results as intention-to-treat analysis.
Statistical analysis
Continuous variables are presented as mean±standard deviation and categorical variables as frequency. Statistical analysis was performed using SPSS 11.5 (SPSS, Chicago, IL, USA).
Results
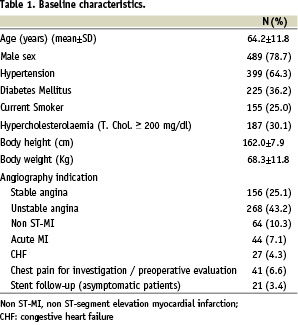
Baseline characteristics and indications for the procedure are shown in Table 1.
Vascular access data and the angiographic findings are shown in Table 2.
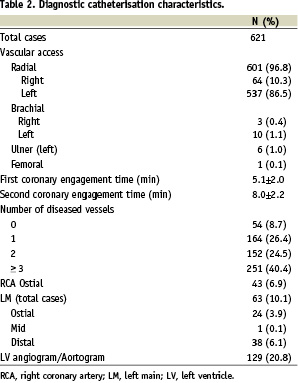
Radial artery was successfully accessed in 601 cases (96.8%). Ikari left 3.5 was used in all cases of crossover from radial to other approaches. No patient had symptomatic local vascular complications, hand ischaemia or nervous complications at the time of hospital discharge or, one week later, at out-patient follow-up. The majority of patients had two or more diseased coronary arteries (Table 3).
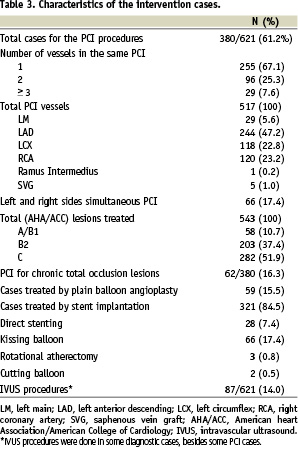
Coronary intervention was performed in 380 (61.2%) patients for 517 vessels and 543 lesions.
Among the PCI cases, 321 patients (84.5%) had 537 coronary stents. Most of the treated lesions were complex (89.3% were AHA/ACC class B2/C). Sixty-two of the PCI patients (16.3%) had chronic total occlusions. Twenty-nine patients (7.6%) had PCI for left main lesions including a single stent in seventeen patients, two stents in eleven patients and balloon angioplasty for a shocked acute myocardial infarction patient with the distal left main as culprit. Intervention of two or more vessels during the same procedure was performed in 125 patients (32.9%), including sixty-six patients (17.4%) with different sides coronaries. Additional procedures included; primary PCI for acute myocardial infarction with adjunctive PercuSurge GuardWire™ distal balloon protection device (Medtronic, AVE, USA) in forty-four patients, renal angiography in twenty-two patients, renal stenting in three patient, lower limb angiography in four patient, and 5Fr-in-6Fr (using 5Fr Heartrail catheter, Terumo, Tokyo, Japan) child-in-mother technique in three patients.
Table 4 shows the results of study endpoints.
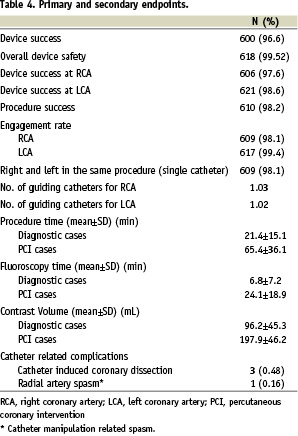
The device achieved 96.6% success rate as efficient single transradial guiding at right and left of coronary arteries in the same procedure. The right transradial procedures represented a small (10.3%) ratio, however, all were successful. The mean number of catheters per procedure was 1.03 for RCA and 1.02 for LCA. In two cases (included as failures) the radial artery were small and allowed only a 5Fr catheter. The overall device safety was 99.52%, as the catheter tip induced RCA dissection in three cases (0.48%). In these cases, two had a short dissection limited to the proximal RCA segment, with pre-existing borderline stenosis at the ostium in one, and mild lesion for the second. Each artery was successfully treated using a single stent. The third RCA had spiral dissection and showed no evidence of atherosclerosis, as proved by intravascular ultrasound. These three cases occurred within the first two hundred cases, with no more complication cases in the last 421 cases, representing the importance of learning curve. The catheter induced radial artery spasm in one patient.
Alternative guiding catheters for the RCA were; JR 4 in eight patients, JR 5 in three patients, Amplatz left-1 in two patients and 5Fr LBT guiding (Boston Scientific, Scimed, Inc. Maple Grove, MN, USA) in two patients. Alternative catheters at the LCA: Kimny mini in one patient, JL 4 in three patients, JL 5 in one patient, XB in two patients and 5Fr LBT in two patients.
Discussion
The main finding of this study is the feasibility of using the single 6Fr IL 3.5 catheter for transradial right and left coronary angiography and intervention when PCI is indicated.
The search for the ideal multi-purpose catheter is not new9,16-18 but, not yet achieved. Using multiple catheters by the transradial approach might cause more patient pain especially during catheter exchange16. Radial artery spasm incidence varies around 10%4,19,20. Catheter exchange might also result in radial artery damage21. Using a single, multi-purpose, catheter for several tasks with high device and procedural success rate is appealing in this study cohort, with substantially less radial artery spasm, vagal syndrome and catheter handling difficulties17 as compared to previous studies5,8. Also, using a single catheter might decrease procedure and fluoroscopy times that might be particularly important to high-volume operators doing multiple procedures, and might add to the cost saving for the transradial approach7,16.
What should be the size of that ideal multi-purpose transradial catheter? The use of larger than 6Fr catheters is one of the limitations of the radial access22. The 5Fr16 and 4Fr18 catheters did not provide advantage compared to 6Fr catheters in radial patency or procedure success23. A mini-invasive strategy with 5Fr guiding can not be adopted for all comers in PCI23,24, or even with much simpler PCI cases compared to the current study. Smaller diagnostic catheters and lower heparin doses have reduced femoral complications as well as the need for prolonged bed rest25. So, the target is a good guiding catheter rather than just a multi-purpose diagnostic one.
This study reports high device and procedural success rates compared to previous studies2,9,22 despite the complexity of cases in terms of clinical indications, vessels and lesions subsets and variety of adjunctive devices used. Despite being a guiding catheter, it also compares favourably with other single diagnostic catheters used for right and left coronary diagnosis16-18,26, or using different sizes of IL for LCA and Ikari right for RCA interventions12. The procedure and fluoroscopy times in our study were shorter than some studies22, and comparable to others9,17,23,27. This study compares favourably to other studies in the number of guiding catheters used9,17,18 and contrast volume used12,18, despite including the longer learning curve of several transradialists and using the IL for some extra-coronary procedures.
Even though originally designed for right transradial approach12,13, in this study, IL 3.5 achieved success rate similar to different sizes of Ikari catheters used by right radial approach12, which is another important finding in our study.
Rationale of the high device success rate for right and left coronaries
The high device success at LCA can be explained by two factors: First, similar to the JL curve, the IL guiding catheter had proven to provide high engagement rate during TRI12,26. Second, good back- up is provided by the greater angle and area of contact between IL and the reverse side of the aorta11,12.
This is the first study that reports using IL for RCA diagnosis and intervention. When the primary curve of the IL catheter is rectified with a guidewire, it resembles the curve of JR catheter26, so it can be used with a high engagement rate. However, the longer first segment with additional length from the second segment as the catheter is rectified, and the larger area of contact with the opposite aortic wall explain the stronger, direct back up provided by IL 3.5 for the RCA.
Right coronary dissection
Right coronary dissection is a common problem for all the multi-purpose strategies17. The overall incidence of RCA dissection in our series is 0.48% (3/621), which is marginally higher than that in other studies28,29. However, Louvard reported comparable incidence of RCA dissection using a left Amplatz catheter for right and left coronary diagnosis17. Compared to JR, IL3.5 might engage deeply and forcefully into RCA, which may cause dissection, especially when the vessel is atherosclerotic. This study started an innovative technique, without preceding instruction to guide us in using the device more safely. The three cases occurred early in the learning curve, representing the importance of a learning curve for safety issues. However, later on more junior transradialists started to use the catheter efficiently and safely guided by the original operators. Still, we emphasise such complications as potential limitations of routine use of guiding catheters for coronary diagnosis until the learning curve is passed.
Limitations of the study
First, the study didn’t have a control arm. Second, the study was vulnerable to subjectivity on the part of different operator’s practice, with its possible implications on procedure time and contrast volume used – however, this is a real world practice. Third, this study reflects a previously unreported experience, with a new application for a novel guiding catheter which might have negatively affected some important outcomes, i.e. complications. Finally, only a small percentage of cases were done via the right radial artery; however, all right transradial procedures were successful.
Conclusion
Transradial right and left coronary catheterisation and intervention using IL 3.5 as a single guiding catheter is feasible in the vast majority of daily practice cases. A learning curve for using the IL 3.5 might be needed for efficient and safe applications.
Online data supplement
Supplementary data
To read the full content of this article, please download the PDF.
Vidéo 1
Vidéo 2
Vidéo 3
