Abstract
Symptomatic non-obstructive coronary artery disease (NOCAD) is an increasingly recognised entity that is associated with poor cardiovascular outcomes. Nearly half of those undergoing coronary angiography for appropriate indications, such as typical angina, or a positive stress test have no obstructive lesion. There are no guideline recommendations as to how to care properly for these patients. Physiologic assessment of the coronary arteries beyond two-dimensional angiography is not standardised, yet it can provide valuable information in patients presenting with typical angina in the setting of NOCAD. In this consensus document, we detail steps for the interventional cardiologist to evaluate the patient with symptomatic NOCAD in the cardiac catheterisation laboratory, first with the assessment of coronary flow reserve (CFR), and then with delineation of deficiencies in non-endothelium-dependent CFR (CFRne) versus endothelium-dependent CFR (CFRe) using provocative agents such as adenosine and acetylcholine, respectively, followed by the evaluation of smooth muscle function with nitroglycerine (NTG). Once the mechanism behind the anginal symptoms is established, one can identify the appropriate treatment strategies to address the physiologic deficiency that is present. Despite an established safety profile, a comprehensive assessment may be considered for selected patients which requires an understanding of the appropriate invasive evaluation by the practising interventional cardiologist when evaluating not only patients with obstructive CAD but also those with NOCAD.
Abbreviations
CAD: coronary artery disease
CFR: coronary flow reserve
CFRe: coronary flow reserve, endothelium-dependent
CFRne: coronary flow reserve, non-endothelium-dependent
CVD: cardiovascular disease
NOCAD: non-obstructive coronary artery disease
NTG: nitroglycerine
Introduction
Conventional angiography visually and subjectively assesses only approximately 5-10% of the coronary vascular resistance1. The remaining 90-95% of the coronary vasculature requires a detailed and systematic approach for successful evaluation of patients with typical symptoms of cardiac angina without obvious obstructive coronary artery disease (CAD). In the visible conduits, an atherosclerotic lesion greater than 70% has traditionally been treated with revascularisation – surgical or percutaneous – for the resolution of symptoms2. Non-obstructive CAD (NOCAD), a recently emerging term3, is defined as less than 50% luminal diameter obstruction4. A plurality of patients undergoing coronary angiography for compelling symptoms or following a positive non-invasive ischaemia test have NOCAD5. Moreover, 50% of such patients who are referred for coronary angiography are found to have coronary endothelial or non-endothelial dysfunction independent of obstructive CAD6. Although there are no specific guideline recommendations, in cases where there is discordance between the patient’s anginal symptoms, non-invasive stress testing, and the coronary luminogram, a comprehensive evaluation may be considered for selected patients with non-significant CAD on angiography or alternatively for research purposes to ascertain treatment and prognostic information.
Here we outline a step-by-step approach to the symptomatic patient with NOCAD by the interventional cardiologist in the cardiac catheterisation laboratory with an emphasis on the characteristics of patients presenting with NOCAD, methodological approaches to evaluate the structure and function of the coronary arteries, how these results should be interpreted/reported, and the resultant therapeutic options.
Physiologic basis of functional coronary assessment
The main role of epicardial coronary vessels is conductance; the key role of the microcirculation is to match blood supply to myocardial oxygen requirements (mostly through modulation of arteriolar tone) and to make possible the interchange of oxygen, nutrients and metabolites between myocytes and blood (performed in the capillary network). The mechanism for ischaemia generation in the epicardial vessels is conductance impairment, mostly caused by inward plaque growth during atherogenesis, intraluminal obstruction caused by thrombus, or coronary spasm. Conversely, microvascular disease results mostly from inadequate coronary arteriolar autoregulation and from structural remodelling of arterioles of the capillary bed, intraluminal plugging, or microvascular oedema/haemorrhage impairing the conductance of the microvasculature.
When assessing the ability of the epicardial vessels and microvasculature to meet myocardial demand, coronary flow reserve (CFR) is the fundamental measure of the ability of the entire coronary circulation to augment blood flow with stress measured as a ratio of maximal coronary blood flow (usually drug-induced) to baseline physiologic blood flow (Figure 1). CFR assessment can be divided into an endothelium-independent component (CFRne) and endothelium-dependent coronary flow (CFRe), described later in the text. Testing for dysfunctional, endothelium-independent coronary microvascular function (CFRne) is accomplished by obtaining a ratio of blood flow or velocities at rest to that at maximal hyperaemia – usually achieved with intracoronary adenosine. In addition, measurements of microcirculatory resistance during hyperaemia may inform the clinician as to the cause of impaired microcirculatory conductance (Figure 1).
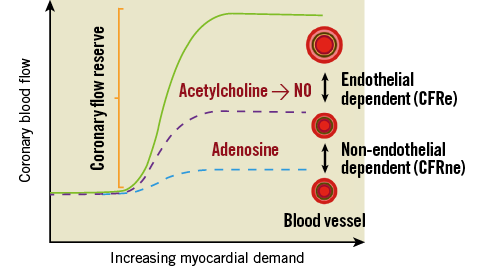
Figure 1. Coronary blood flow response to increasing myocardial demand. Increasing myocardial demand leads to an increase in coronary blood flow (CBF). The ratio of CBF above baseline is referred to as coronary flow reserve (CFR) and is composed of an endothelium-independent component (CFRne) and endothelium-dependent component (CFRe).
CFRne can be measured with intracoronary Doppler techniques using blood cell velocity as an approximation for flow based on Poiseuille’s law of fluid dynamics. A typical coronary Doppler tracing is shown in Figure 2. It assesses the perfusion capabilities of the macrocirculation and microcirculation. In normal individuals, CFRne is above three and can be as high as five indicating that the coronary circulation can normally increase perfusion up to five times basal levels if provoked by physiologic, pharmacologic, or pathologic stressors. However, CFRne can be reduced in a wide variety of diseases such as obstructive CAD, coronary vasospasm, hypertension, left ventricular hypertrophy, and even valvular heart disease.
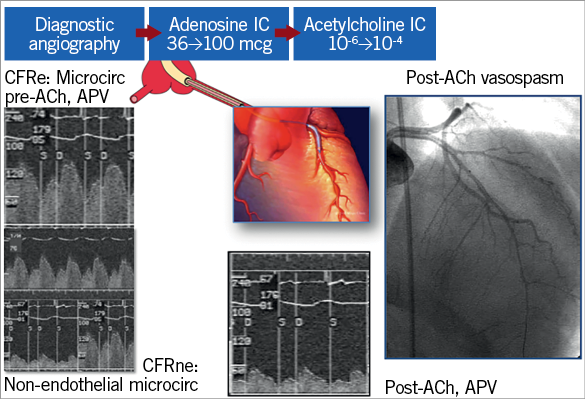
Figure 2. Functional angiogram protocol. Typical functional angiography demonstrating coronary flow reserve (CFR) changes in an endothelium-dependent (CFRe) and endothelium-independent (CFRne) manner. The protocol, initiated with diagnostic angiography and moving on to adenosine and acetylcholine (ACh) infusion, is depicted on top. CFRne is assessed using blood flow velocity profiles (average peak velocity [APV]) at rest and after adenosine infusion (bottom middle). Assessment of CFRe is depicted on the far left with a normal pre-ACh reading consisting of a predominant diastolic component on the top. The lower left panel shows a marked reduction in APV after the infusion of ACh indicative of poor microvascular recruitment of blood flow seen in patients with microvascular disease. The angiogram (far right) shows an example of vasoconstriction after the administration of ACh.
Initial evaluation
The epidemiology and initial evaluation comprise a history and physical, lab evaluation, ECG, non-invasive imaging, and initial diagnostic catheterisation. This is detailed in Supplementary Table 1.
Protocol for functional coronary artery assessment
The functional assessment of the microcirculation has been extensively studied and described previously6-9 (Supplementary Table 2). Testing can be done ad hoc during the patient’s initial coronary angiogram, or in a staged fashion after the initial angiogram if conditions are not favourable for proceeding with further invasive assessment (radial spasm, confounding intra-arterial vasoactive medications, ACS, etc.). Ideally, the majority of, if not all vasoactive drugs should be withheld prior to testing – particularly nitrates and calcium channel blockers. Other vasoactive substances such as nicotine and caffeine should also be withheld for 24 hours prior to testing. Furthermore, operators experienced in performing and interpreting these tests can be consulted in the study of these patients so that technical success is maximised in addition to arriving at a proper diagnosis.
VASCULAR ACCESS
In patients without obstructive CAD, as determined by FFR/iFR, where invasive physiologic assessment is indicated, one must carefully plan the procedure including the equipment used (Figure 3, Figure 4), vessel studied, and order of assessments. Traditionally these cases are performed from a femoral approach. This is considered best for two main reasons. The first is to avoid the need for vasodilators routinely administered during radial access. Secondly, there is concern for radial artery spasm with the potential need for the administration of vasodilatory agents which may confound the results.
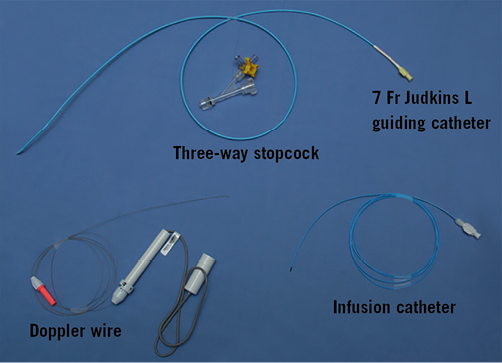
Figure 3. Equipment used in functional angiography including guide catheter and second three-way stopcock (top), 3 Fr infusion catheter (bottom right), and Doppler wire (bottom left).
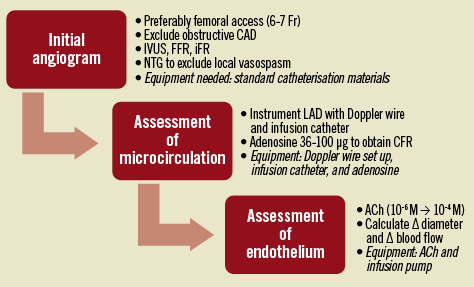
Figure 4. Clinical protocol for NOCAD. Suggested order of catheterisation procedures and equipment required for each step in the process.
STUDY ARTERY
Unless otherwise indicated by regional abnormalities on a non-invasive stress test, the left anterior descending artery (LAD) is the conventional vessel of choice for these studies as this vessel has been most commonly studied. This vessel subtends the most myocardium, is typically very approachable with the equipment due to its large calibre, and can be assessed easily in terms of Doppler velocities and quantitative diameter assessments. The left circumflex or right coronary arteries can be studied if inferior or lateral changes are seen on the non-invasive test or if transient ischaemic mitral regurgitation secondary to posterior or lateral ischaemia is in question. If these arteries are to be studied, changes in guiding catheter selection may need to be made in addition to reductions in dosing of provocative medications.
Equipment
A 7 Fr guide is predominantly used. This is typically an extra back-up (EBU/XB) or Judkins left shape depending on the anatomy (Figure 3, Figure 4). Recently, the increasing popularity of the radial approach and the ability to utilise a 7.5 Fr sheathless guide or 7 Fr radial sheaths and guides has allowed these procedures to be performed using the radial approach. More data are needed to confirm that the radial approach is safe and effective to use. To avoid catheter or wire thrombosis, IV heparin should be administered at a standard dose (60-80 IU heparin/kg body weight) to ensure an activated clotting time (ACT) greater than 250 seconds. An additional safety measure is having a syringe for intra-arterial nitroglycerine (NTG) easily available should coronary spasm occur unexpectedly.
Once the 7 Fr guide is positioned within the ostium of the left main coronary artery, the Doppler wire and infusion catheter are positioned in the mid portion of the vessel. As the Doppler wire is not as manoeuvrable as a workhorse coronary wire, it is possible to use a soft-tipped coronary guidewire initially, over which the infusion catheter can be advanced to the appropriate position within the artery. The workhorse wire can then be exchanged for the Doppler wire, which should be positioned just distal to the tip of the infusion catheter required for concomitant intracoronary drug delivery. The infusion catheters typically used include the RapidTransit catheter 2.8 Fr (proximal), 2.3 Fr (distal), 150 cm length, internal diameter 0.021” (Codman Neuro, Johnson & Johnson, New Brunswick, NJ, USA) or Slip-Cath® Infusion Catheter 3.0 Fr, 150 cm length, internal diameter 0.025” (Cook Medical, Bloomington, IN, USA) (Figure 3). The infusion catheter should be positioned at the proximal to middle portion of the vessel (if the vessel is large enough to accommodate it without creating ischaemia) to ensure adequate drug delivery to the distal portion of the artery with plenty of upstream vessel not directly affected by the drug infusion in order to test upstream flow-mediated vasodilation. The infusion catheter could still be used if the artery in question is the right coronary artery to evaluate upstream and downstream acetylcholine (ACh) effects on the artery. We recommend attaching, through a second three-way stopcock delivery system (Figure 3) set up outside of the body, an infusion pump able to deliver ACh at 1 ml/min in increasing concentrations, as shown in Figure 2. This proposed protocol (Figure 4) has demonstrated excellent safety in observational studies and randomised trials6,10,11.
Functional assessment protocol
Once the vessel has been successfully instrumented with the infusion catheter, one can carefully position the Doppler velocity wire through the infusion catheter into the vessel being studied. Two available 0.014” Doppler wires can be used – either the ComboWire® or the FloWire® (both from Philips Volcano, San Diego, CA, USA) (Figure 3). Both wires have been independently tested and verified for safety and reliability in assessing coronary Doppler signals to obtain coronary velocity data6-8,10,11. The Doppler wire must be carefully placed and positioned within the coronary artery to avoid poor Doppler data quality. Subtle movements of the Doppler wire or infusion catheter to improve data quality must be made with extreme care in order not to damage the vessel. Repositioning of the equipment, if required, should be done using the workhorse wire to reposition the infusion catheter before re-inserting the Doppler wire.
Once the testing is ready to begin, the guide and infusion catheter should both be properly flushed with heparinised saline and equalised. The system should not be pre-treated with intracoronary NTG, as this will alter blood flow independent of the endothelium or microcirculation with the smooth muscle-directed vasodilation.
An alternative to an infusion catheter placed locally in the coronary artery is to advance the flow wire into the vessel without the use of an infusion catheter and to infuse the drug directly through the guide. This protocol variation can be considered if the clinical question can be answered by simply administering adenosine to measure Doppler velocities, obtaining a CFRne or testing for epicardial spasm with an ACh bolus. Whilst overall it is safe to perform, there is a risk of left main or proximal vessel dissection with this method, not to mention the possibility of vasospasm throughout the left-sided coronary arteries without placement of workable coronary wires in the distal vessels.
ENDOTHELIUM-INDEPENDENT MICROVASCULAR BLOOD FLOW – CFRne
It is recommended to begin by obtaining CFRne once the Doppler wire and infusion catheter are both in place. The administration of intracoronary adenosine (intravenous adenosine can produce unwanted and confounding systemic hypotension12) allows the measurement of maximal coronary endothelium-independent vasodilation. Depending on the artery of choice, a dose of 36 to 100 mcg is preferred (Figure 2, Figure 4). The hyperaemic average peak velocity (APV) is compared to the resting APV, and a CFRne ratio is obtained (Figure 2). This should be repeated two to three times until a stable maximal APV is obtained.
ENDOTHELIUM-DEPENDENT MICROVASCULAR BLOOD FLOW – CFRe
Once the assessment of the non-endothelium-dependent microcirculation has been ascertained via adenosine administration and the CFRne obtained, the next step in the workup of patients with NOCAD is to assess the endothelium-dependent epicardial diameter and microcirculation, CFRe (based on changes of APV) with the administration of the endothelium-dependent vasodilator ACh. This will assess the endothelium-dependent vasodilatory properties of the epicardial as well as the coronary microvasculature. Two measurements are needed to assess CFRe – the APV and the coronary artery luminal diameter.
Maintaining the stable positioning of the infusion catheter and with the Doppler wire in place, graded infusion of ACh administration should be initiated with increasing doses of ACh (10-6 M → 10-4 M; or equivalently, ACh 0.001 mmol → 0.1 mmol) for up to three minutes at 1 ml/min via an infusion pump. The infusion should be quickly stopped should symptoms or complications occur. During the infusion, concomitant measurement of epicardial diameter via quantitative coronary arteriography (QCA) using any angiographic imaging software and APV will allow calculation of coronary blood flow (CBF). The purpose of this testing is twofold: 1) assessment of coronary epicardial vasoconstriction, and 2) assessment of the ability of the endothelium of the coronary microcirculation to increase CBF appropriately. This particular protocol involves the measurement of coronary epicardial diameter at three sites along the artery five mm proximal, five mm distal to the infusion catheter for CBF calculations (usually mid vessel), and at the distal vessel as well as APV after three minutes of each ACh dose infusion. At the conclusion of the ACh infusions, or should ischaemic symptoms occur during ACh infusions, 100-200 mcg of intracoronary NTG should be delivered via the guide catheter. Haemodynamic data as well as patient symptoms should be assessed at baseline, the end of each three-minute period of infusion, and after the administration of the intracoronary NTG. Some operators will choose to administer ACh, then NTG, and finish with adenosine to obtain CFRne with the thought being to remove epicardial vessel tone with NTG prior to adenosine. Both protocols have been used and reported with comparable results13.
Once the coronary diameter and APV have been recorded at each ACh dose, a large dose of ACh (100 mcg of 10-4 M) can be administered while measuring the degree of change in epicardial coronary diameter to rule out coronary vasospasm if there are no contraindications to the large intracoronary bolus of ACh. This approach is safer than the traditional means of assessing coronary vasospasm with methylergonovine14. There is also the risk of refractory15 or multivessel spasm during this provocative test16. As there is a guiding catheter and coronary guidewire in place, intracoronary NTG or balloons can be delivered to resolve cases of severe spasm. An in-depth review of the medications used in these assessments is included in Supplementary Appendix 1.
An alternative method to assess the coronary microcirculation, based on coronary thermodilution techniques, is the index of microcirculatory resistance (IMR). This technique uses distal coronary pressure divided by changes in intracoronary temperature measurements (proximal to distal) to approximate coronary resistance17. IMR has been shown to be independent of epicardial vascular function, reproducible, and has even been evaluated in STEMI patients, providing important prognostic information regarding ventricular function at three months18. Despite reasonable prediction of events and outcomes following percutaneous coronary intervention19, as there are no established reference values for IMR there are no guideline-based recommendations for its regular utilisation in the catheterisation laboratory.
Standard for interpretation/reporting of the test results
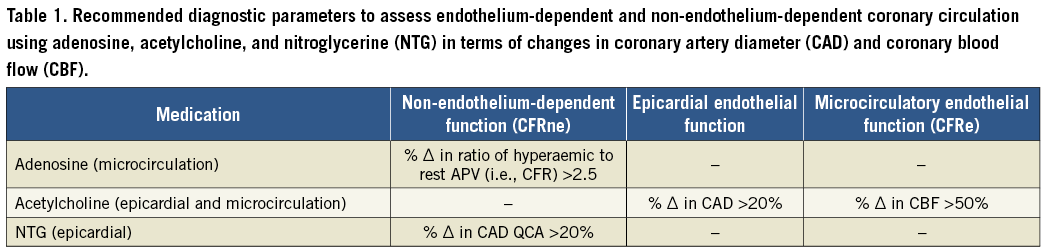
To assess the coronary circulation with ACh administration, we propose the following parameters for the diagnosis of epicardial vs. microvascular dysfunction. Often the diagnosis of epicardial spasm can be made without specific calculations and with the combination of drastic angiographic vasospasm and reproduction of symptoms with ACh administration; however, one should be careful to calculate changes in CBF as changes in diameter might not alter distal microvascular flow. Coronary diameter can be measured via any standard catheterisation laboratory imaging software, and should be measured proximal to the infusion catheter, 5 mm distal to the site of ACh administration, and in the distal vessel. CBF can be calculated from measurements of coronary flow velocity and coronary cross-sectional area with the modified hydraulic equation CBF=0.5×velocity×area. Using the metrics obtained during testing, CBF=0.5×APV×(radius2×π). Coronary radius (diameter/2) and CBF obtained at the site and distal to the site of ACh administration assess the direct endothelial response to ACh, while the diameter and CBF proximally assess the ability of the vessel to respond to increases in blood flow. This should also include vasodilation and increase in CBF. An increase in coronary diameter of greater than 20% and/or an increase in flow over 50% are considered normal (Table 1)6-9.
The operator should communicate the presence of CAD and degree of atherosclerotic burden, the endothelium-dependent and non-endothelium-dependent behaviour of the microcirculation to respond to physiologic challenges, as well as notation describing the baseline APV in the vessel studied, maximum CFR obtained, the dosing of adenosine, and any symptoms (Figure 5). Additionally, the report should also state whether spasm was present or not, and the degree of vasodilatory response of the vascular smooth muscle to NTG. Presenting the specific vascular pathology related to the symptoms is an important piece of information to pass along to the referring provider as it provides insight into targeted medical therapies.
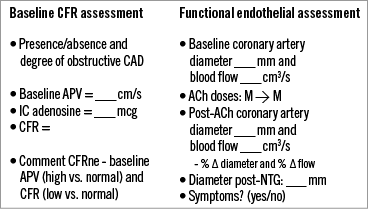
Figure 5. Functional assessment report. Typical report with step-by-step interpretation of the data for coronary functional testing.
The report should also include the percent changes in coronary diameter and CBF at the site of infusion as well as proximally with increasing ACh administration. One should report the maximum percent changes in diameter and CBF. This will allow commentary on the epicardial response to ACh in terms of vasospasm, as well as the CBF response, in order to report any endothelial microvascular dysfunction. Finally, the report should include any symptoms reported by the patient to see whether the provocative ACh testing reproduced any of the patient’s angina symptoms.
Suggested therapies
There is an absence of large, randomised clinical trials aimed at addressing therapeutic options for these patients; many of the trials focus either on symptom relief or on improvement in physiologic coronary blood flow. However, there are limited data demonstrating benefit in treating these patients20; upcoming studies do target such a population21. Therefore, most of the treatment strategies for NOCAD – similar to obstructive CAD – should focus on basic cardiovascular prevention principles such as weight loss, diet22, and exercise23. In addition to lifestyle modification, there are limited data supporting pharmacologic agents as improving symptoms and physiology (Figure 6), and individual agents as outlined specifically in previous publications24,25. Finally, consideration should be given to the establishment of a dedicated chest pain clinic to formalise procedures and protocols for the evaluation of chest pain, to establish best practices for ongoing and long-term treatment for symptoms, and to provide a consistent follow-up for these patients.
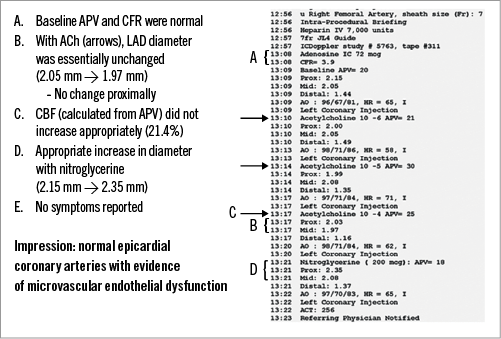
Figure 6. Functional assessment report example. Proposed treatment log for non-obstructive CAD including vasodilators, both epicardial and microcirculatory, as well as non-vasodilatory therapies.
Conclusions
This document should serve as a guide for evaluating patients with symptomatic non-obstructive CAD. These comprehensive assessments are safe and have been intricately designed at certain centres for diagnostic or research consideration for selected patients found to have NOCAD on angiography. Beginning with the initial workup involving history and physical, laboratory, and potentially non-invasive imaging, the next step is the exclusion of obstructive CAD based on coronary angiographic, physiologic, and imaging assessment. Although there are no specific guideline recommendations to guide testing, once obstructive CAD is eliminated, the coronary microcirculation is evaluated in a standard way with appropriate protocols and equipment. This is accomplished with the administration of intracoronary adenosine, ACh, and NTG to obtain non-endothelial coronary function (CFRne), endothelium-dependent coronary function (CFRe), and to evaluate epicardial vasospasm and smooth muscle function. With these simple strategies, one can safely and effectively evaluate and care for those patients with NOCAD.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Supplementary Appendix 1. Further background information.
Supplementary Table 1. Preliminary NOCAD workup prior to functional angiogram including history and physical, lab analysis, imaging, non-invasive testing, and diagnostic angiography.
Supplementary Table 2. Recommended protocol for coronary provocative testing in the cardiac catheterisation laboratory.
To read the full content of this article, please download the PDF.