The 2017 annual meeting of the EuroCTO Club in Berlin was the biggest ever in the history of this congress which has now reached its 9th edition. The 350 active medical participants reflect the growth of the Club, with 182 full members and 114 associate members, an increase of almost 100 physicians in one year (Figure 1).
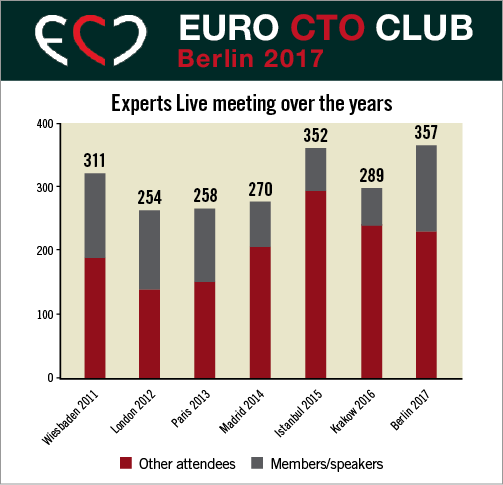
Figure 1. Increasing number of members, speakers or other attendees at the EuroCTO Club Experts Live Meeting in the last seven years.
The nine “Live” cases were all successful and were performed by CTO expert operators from Europe, Japan and North America in the prestigious Charité University Clinic Benjamin Franklin in Berlin, supported by the local team of Ulf Landmesser and Alexander Lauten.
Live cases and technical discussion around the various procedural steps were the focus of the meeting; however, these are also the most difficult part to summarise. Case presentations and discussion were recorded and are available on the club website (www.eurocto.eu). The meeting offered an opportunity to appreciate similarities and differences of approach to complex coronary occlusions among Japanese, US and European physicians.
We started with anterograde cases to highlight the basic wire approach, and then more complex cases were presented, requiring a combined anterograde and retrograde approach. In selected cases with obvious ambiguity of the proximal cap or truly ostial RCA occlusion, retrograde was the primary choice, used in five out of the nine cases transmitted. This allowed appreciation of the superior performance of dedicated wires (SUOH03 and SION® black; both Asahi Intecc, Aichi, Japan) recently added to the classic highly steerable and delicate SION wires (Asahi Intecc), and of smaller microcatheters (Corsair Pro and Caravel [both Asahi Intecc], and Turnpike® LP [Teleflex/Vascular Solutions, Minneapolis, MN, USA]). These microcatheters compensate for their limitation in strength and inability to advance through rotation with a very small profile, increasing safety in tortuous epicardial collaterals and facilitating the use of a 6 Fr radial approach. Dual lumen catheters (FineDuo® [Terumo, Tokyo, Japan], NHancer RX [IMDS, Roden, the Netherlands], Twin-Pass Torque [Teleflex/Vascular Solutions]) were used liberally and for multiple different purposes, i.e., puncture with greater support of the proximal occlusion cap having the distal tip of the catheter parked in a side branch, negotiation of a second wire to the distal end of the occlusion when the first went subintimal, and access to side branches at the site of the distal re-entry.
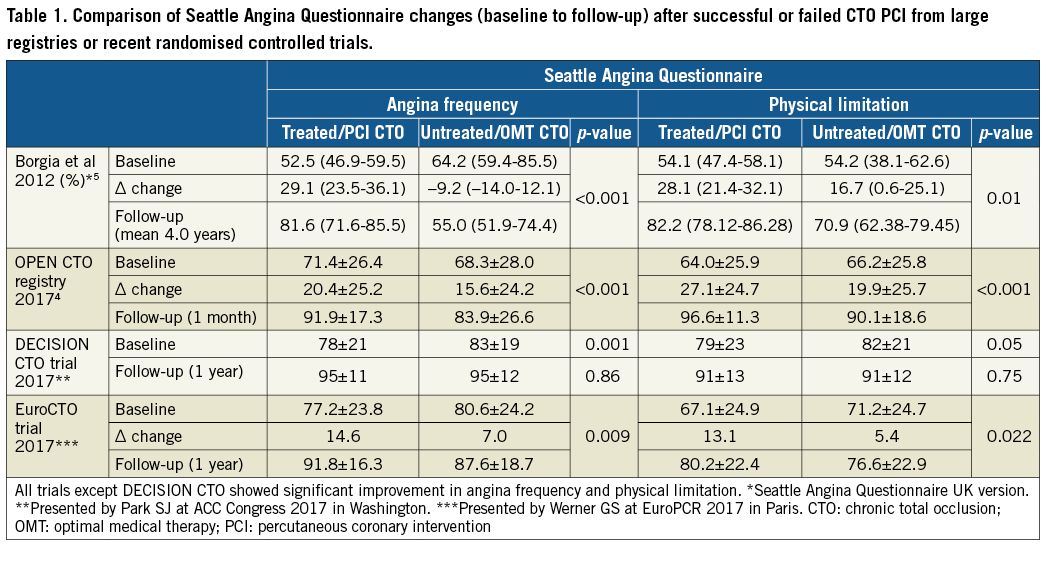
Dedicated lectures raised interest and sparked discussion in between cases. David Hildick-Smith added a novel index (to the classic J-CTO score and CL and PROGRESS scores1) to predict success derived from the more than 15,000 entries of the EuroCTO database. The review of the CTO literature in the last year, assigned to Carlo Di Mario, showed that in modern practice CTOs are probably more frequent than the 15-20% incidence reported in old studies. The 111,273 patients with coronary artery disease studied in Veterans Affairs hospitals2 from 2007 to 2013 (mean age 64.7 years) showed an incidence of 26.4%. CTO PCI was attempted more often than in previous series (8.1%), and procedural success was higher (79.1%). In this large registry, there was also a significant two-year-mortality reduction between successful and failed PCI patients (unadjusted odds ratio [OR] 0.62, CI: 0.45-0.85, p=0.03; adjusted OR 0.67, CI: 0.47-0.95, p=0.02). This obviously questions the absence of mortality differences in the three recently completed randomised trials (EXPLORE3, DECISION CTO [Park SJ. Optimal Medical Therapy With or Without Stenting For Coronary Chronic Total Occlusion. NCT01078051. Presented at American College of Cardiology Congress, Washington, DC, March 2017], and EuroCTO [Werner GS. A Randomized Multicentre Trial to Evaluate the Utilization of Revascularization or Optimal Medical Therapy for the Treatment of Chronic Total Coronary Occlusions. NCT01760083. Presented at EuroPCR, Paris, May 2017]). Gerald S. Werner commented that the first and last of these trials were too small and had too short a follow-up to expect differences in hard endpoints. In DECISION CTO there was the possibility to treat non-occlusive lesions after randomisation and this, together with the high crossover rate (18%) and the exclusion of highly symptomatic patients as shown by the small percentage of CTOs enrolled in the trial compared to the total number treated in the participating centres, explained the similar adverse event rate. The 1,000 patients in the US OPEN CTO registry4, consecutively enrolled and independently monitored, demonstrated a high success rate of 81% (cath lab adjudication) with improvement of all the components of the Seattle QoL questionnaire after one month in the successful cases (from 49.5±27.5 to 76.1±21.4, p<0.01), confirming the primary endpoint reached in the EuroCTO trial.
All trials and registries compared in Table 1, except DECISION CTO, showed significant improvement in angina frequency and physical limitation (Seattle Angina Questionnaire) after successful CTO PCI. This difference can be explained by the use of the absolute difference in angina frequency and physical limitation with a significantly worse baseline level in the PCI group, together with the high crossover rate and the confounding effect of non CTO-PCI in multivessel-disease patients. In the OPEN CTO registry, the higher than expected complication rate, especially perforations requiring treatment (4.8%), might be an effect of the greater scrutiny of an independent monitoring and event adjudication but may also be caused by the aggressive hybrid strategy with 24.3% of the cases which were finally successful completed using anterograde dissection reentry (Stingray™ LP; Boston Scientific, Marlborough, MA, USA).
The SYNTAX II6 594-patient registry presented by the principal investigator Javier Escaned at the 2017 ESC Congress in Barcelona showed that a successful CTO recanalisation was much more frequent with today’s techniques (87%) than with the techniques used 10 years ago in the original SYNTAX trial (53%). This certainly contributed, together with the consistent use of physiology and IVUS guidance and of the SYNERGY™ stent (Boston Scientific), to bringing down the MACE rate at two years, 8% lower than in matched lesions in SYNTAX.
The specificity of recanalisation of saphenous vein grafts (SVGs) and of native arteries through occluded SVGs was optimally illustrated by Joachim Büttner. Results of bioresorbable vascular scaffolds (BVS) in CTO recanalisation showed a similar outcome of 153 CTO lesions treated with BVS vs. 384 treated with second-generation metallic drug-eluting stents (DES), with only a slight non-significant trend to increased stent thrombosis in the BVS group7. Bernward Lauer emphasised the impact of the presence of a CTO in acute coronary syndrome (ACS) patients on mortality, acutely and in the long run.
Japanese CTO experts gave a glimpse into a novel CTO technology, the PlasmaWire™ System (RetroVascular, Pleasanton, CA, USA)8. In this device two wires can be connected to a radiofrequency generator and deliver energy at the tip to simplify the completion of the reverse CART technique or to facilitate penetration of a hard proximal cap in the anterograde approach.
A new and important feature of this year’s course was the implementation of lectures in CTO PCI for young beginners. CTO experts dedicated their lectures to CTO basics such as the anterograde approach - how to start, which lesion to start with, which material, which setting, how and when to switch to the retrograde approach (Kambis Mashayekhi), ending with the top 10 lessons learned (Gerald S. Werner).
The general impression at the end of the course was that individual differences among operators have narrowed but there is still a different philosophy in Japan, focused on wire skills and liberal use of IVUS, and paying great attention to maintaining an intravascular course, and in the USA, Canada and the UK, all following an updated version of the hybrid approach with a rapid switch to retrograde knuckling or dissection/re-entry when the anterograde approach does not show rapid progress. The EuroCTO group seems to follow an intermediate course. Despite the differences, with the use of dedicated material and techniques in the hands of experienced operators, success rates as high as 85-90% or more can be expected in very complex CTOs.
The time and venue of the next EuroCTO Club “Live” Workshop 2018 has been announced. It will be on 28-29 September 2018 in Toulouse, France.
Conflict of interest statement
R. Garbo is a consultant for Terumo, Boston Scientific, Volcano, and IMDS. The other authors have no conflicts of interest to declare.