Excimer laser coronary atherectomy (ELCA) is a percutaneous technique developed to modify atherosclerotic plaques using ultraviolet laser energy. Initially conceived to overcome the limitations of conventional balloon angioplasty, coronary laser gained early attention in the 1980s. Early trials with infrared laser systems were hampered by excessive heat-related vascular injury and limited clinical success. The transition to xenon chloride excimer laser technology, which emits pulsed, ultraviolet light with minimal thermal spread, marked a turning point by enabling more controlled plaque ablation1. ELCA has undergone a quiet but impactful renaissance in contemporary percutaneous coronary intervention (PCI). Once considered a niche bailout therapy with limited adoption following early trials, ELCA has re-emerged as a valuable tool in complex lesion subsets, mainly in the setting of “balloon failure” (balloon-uncrossable or -undilatable lesions) and thrombotic lesions1. Improvements in catheter technology, faster and more user-friendly console setup, broader operator expertise, and better procedural strategies have expanded its use far beyond the original indications. In contemporary PCI, ELCA has also demonstrated consistent efficacy, with favourable short- and long-term outcomes23. The procedural framework known as the “5 Ss” rule, originally detailed by Egred and Brilakis1 (Selection of patients, Size of catheter, Settings, Saline flush protocol, and Slow advancement), has been used to optimise procedural success. However, this classic concept may benefit from being revisited in light of the evolution of the technique and operator experience during recent years. In this viewpoint, we propose a pragmatic reinterpretation of the original “5 Ss” model. While several of the original principles remain relevant, albeit often modified in daily practice, we also suggest incorporating 3 additional “Ss” representing concepts that have proven to be particularly useful in contemporary ELCA: “Second guidewire compatibility”, “Support”, and “Sense early – switch wisely”.
Readaptation of the classic “5 Ss” in contemporary practice
The first “S”, Selection of patients, initially emphasised cautious use of ELCA in specific scenarios. Nowadays, ELCA’s main indications are balloon failure (balloon-uncrossable or balloon-undilatable lesions), stent restenosis, and intracoronary thrombosis. ELCA can modify both superficial and deep calcium and is effective in treating stent restenosis due to neointimal hyperplasia and calcified neoatherosclerosis. Moreover, by reducing thrombus burden and vaporising thrombotic material, ELCA is useful in acute coronary syndromes with large thrombus burden, stent thrombosis, and saphenous vein graft thrombosis14. While no absolute contraindications exist, early literature listed unprotected left main (LM) disease as a relative contraindication1. Today, ELCA is increasingly used in LM PCI, particularly because it allows simultaneous protection of side branches with a second guidewire. In addition, while moderate calcification was originally listed as a favourable indication, its use in severely calcified lesions has been controversial for years. Emerging evidence now supports the use of ELCA in this scenario. This includes truly uncrossable lesions, peristent calcium contributing to stent underexpansion4, or lesions that combine calcium and thrombus. Caution is still warranted in small-calibre vessels and severely tortuous segments where procedural risks are higher and operator experience is critical.
The second “S”, Sizing of catheter, originally recommended a laser catheter no larger than two-thirds of the reference vessel diameter to reduce the risk of vessel injury. While this remains prudent, current practice has evolved towards lesion-specific catheter choice. The 0.9 mm catheter is the most used due to its excellent deliverability, particularly in balloon-uncrossable lesions. In addition, it achieves 80 mJ/mm2 and 80 Hz and works with a more comfortable on-off time (10-5 seconds) unlike the other catheters (5-10 seconds). Although at first sight it may be considered the most powerful catheter, since the energy is applied in a localised area (fluence), larger catheters may have a more potent effect. Thus, the choice of catheter size should be guided not only by the vessel diameter but also by the type of lesion and procedural goals; so, in lesions located at the LM or proximal segments, larger ELCA catheters may be preferred.
The third “S”, Settings, originally recommended a stepwise increase from default machine calibration values. Nowadays, operator preferences vary significantly: some initiate lasing at maximum fluence and frequency, especially in highly resistant plaques, while others maintain a conservative approach. This heterogeneity reflects real-world adaptation rather than deviation from protocol, making this “S” less prescriptive than initially thought.
Saline flushing, the fourth “S”, was promoted as a safety measure to minimise cavitation effects caused by laser interaction with blood or contrast. This remains the manufacturer-recommended standard. However, newer data and clinical experience suggest that allowing laser interaction with contrast or blood, rather than saline alone, may enhance its efficacy particularly in resistant calcified lesions or stent underexpansion. While this off-label approach should be limited to certain scenarios and experienced operators, it demonstrates how the strict “saline-only” rule is no longer universal.
The final “S” is Slow advancement. Among the original “5 Ss”, this is the only principle that has not required adaptation and continues to be crucial during ELCA. Advancing the catheter at <1 mm/sec remains essential to ensure effective and safe ablation.
The new “Ss”: refined principles for complex PCI
We propose 3 new key principles for a safe and effective use of ELCA (Figure 1).
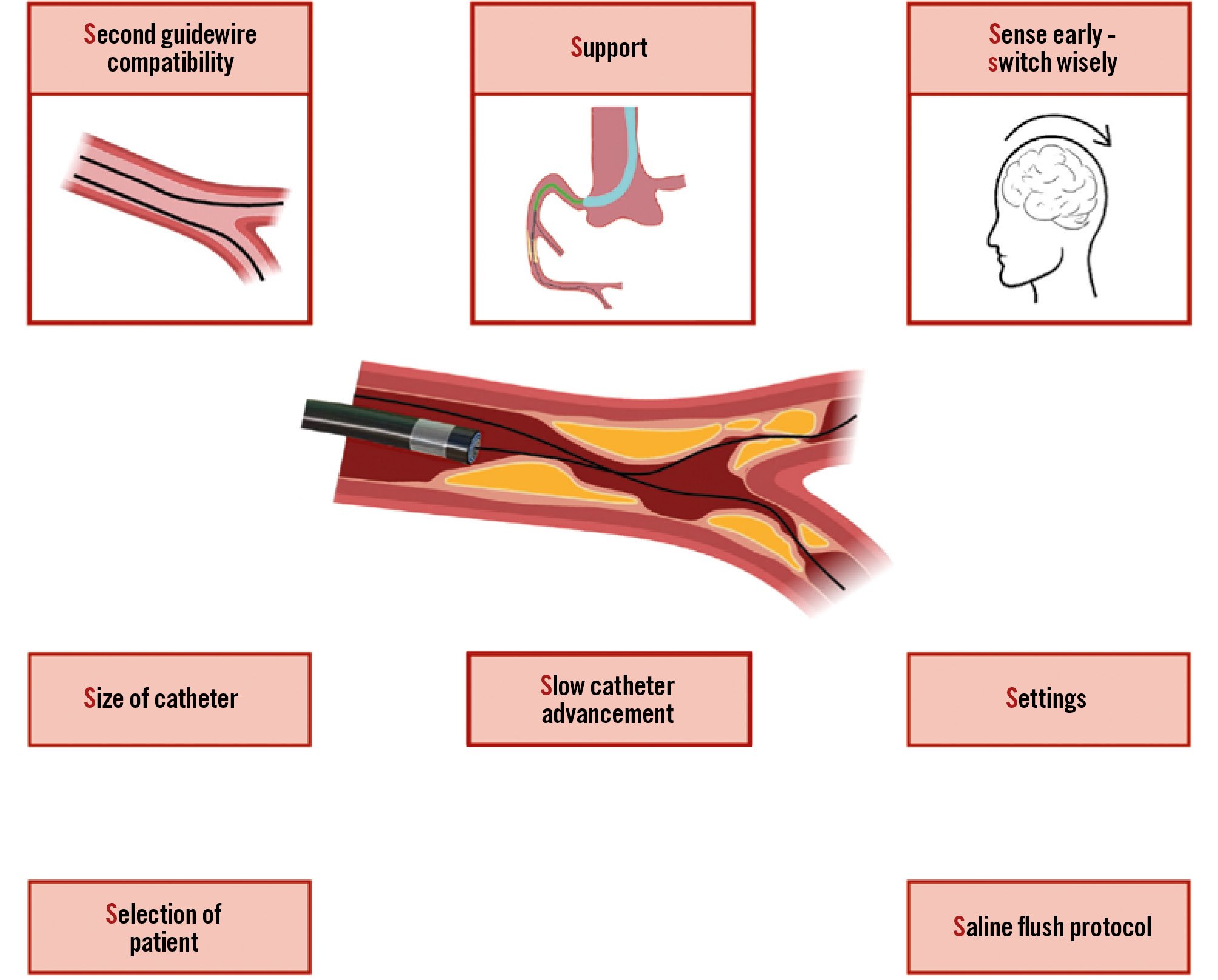
Figure 1. Key principles for safe and effective ELCA: from the “5 Ss” rule to the “new 3 Ss”. This conceptual framework summarises the essential principles for contemporary use of ELCA. The original “5 Ss” rule is revisited and “3 new Ss” are proposed: (1) “Second guidewire compatibility” allows side branch protection and facilitates complex bifurcation strategies; (2) “Support” ensures coaxial alignment and controlled energy delivery, minimising the risk of vessel injury; (3) “Sense early – switch wisely” emphasises lesion assessment and microadjustments to control plaque modification as well as the prompt indication to switch to an adjunctive technique if technical success is not achieved. ELCA: excimer laser coronary atherectomy
1. Second guidewire compatibility
A unique advantage of ELCA compared to other atherectomy modalities is its compatibility with any 0.014” guidewire, but ELCA should be used cautiously with polymer-jacketed wires1. In addition, ELCA can be used in the presence of a second wire and permits effective protection of side branches during laser ablation in bifurcation lesions. This feature supports the execution of complex bifurcation strategies, including LM PCI.
2. Support
Adequate support is essential for safe and effective ELCA. Insufficient support may hinder advancement of the ELCA catheter through the lesion. Optimal guiding catheter selection is essential. Unlike other atherectomy techniques, the use of additional wires or anchoring techniques are feasible with ELCA. Additionally, guide catheter extensions not only enhance support but also facilitate proper and focused infusion of saline or contrast at the target site during lasing.
3. Sense early – switch wisely
Unlike other plaque modification techniques, where technical success is more immediately recognisable (e.g., burr crossing in rotational atherectomy or balloon expansion in intravascular lithotripsy), the effect of ELCA may be less evident, requiring a continuous assessment of the lesion’s response from the beginning of the procedure (“Sense early”). Operators should avoid both abandoning the technique prematurely and trying to force it too much. Alternating gentle forward and backward catheter movements, rather than lasing at a stationary point, can progressively modify the lesion. In some cases, even when the catheter does not fully cross the lesion, sufficient plaque modification is obtained which may allow subsequent balloon crossing and expansion. Additional techniques such as the combination of ELCA with rotational atherectomy (known as RASER)1 or intravascular lithotripsy (ELCA-Tripsy)5 may be required in particularly resistant calcified lesions. Thus, procedural experience is critical in determining when more ELCA pulses are needed or when to switch to alternative plaque-modifying techniques with synergistic effects combined with ELCA (“Switch wisely”).
Having revisited the traditional “5 Ss” framework for ELCA, we believe that while “Slow advancement” remains a central principle for laser success, the other original components benefit from reinterpretation in light of contemporary practice. To enhance this classic model, we advocate for the integration of three additional concepts (“the new 3 Ss”) that have proven particularly useful in real-world complex PCI: “Second guidewire compatibility”, enhanced “Support”, and the crucial ability to “Sense early – switch wisely”. These principles synthesise operator experience and technological advances accumulated over years of practice, tailoring ELCA strategies to specific anatomical and procedural challenges.
Acknowledgements
We would like to thank Mohaned Egred and Emmanouil S. Brilakis for their valuable help in preparing this manuscript.
Conflict of interest statement
A. Jurado-Román is a proctor for Abbott, Boston Scientific, World Medica, and Philips; has received consulting fees from Boston Scientific and Philips; and has received speaker fees from Abbott, Boston Scientific, Shockwave Medical, Philips, and World Medica. M. Basile reports receiving research funding from IHT, outside of the submitted work.