Abstract
Introduction: In interventional cardiology an increasing demand to treat complex coronary lesions (i.e. distal lesions, tortuous vessels, chronic occlusions) has developed within the last years. New devices to fulfill this demand are therefore needed.
Methods and results: The magnetic navigation system (Niobe™ System; Stereotaxis Inc.) represents a novel system which allows 3-dimensional control of the guide wire tip using magnetic fields. Two computer controlled permanent magnets on each side of the patient create a uniform magnetic field which can freely be directed. A small magnet at the guide wire tip will align according to the vector of the magnetic field. Advancing and retracting of the wire is to be done manually. The remaining steps of angioplasty (i.e. balloon angioplasty and stent implantation) are performed conventionally, after magnetically guided crossing of the target lesion.
The study was performed to proof the feasibility of the technique in the treatment of coronary lesions. Seventy seven patients with 82 coronary lesions underwent magnetic guided coronary interventions. Sixty three lesions (77%) could be crossed successfully using magnetic guidance, 13 more by switching to conventional guide wires. Successful angioplasty (with or without stent implantation) was achieved in 74 lesions (90%). Mean fluoroscopy time was 13,9±8 min.
Conclusions: The use of magnetic guidance in coronary interventions is a promising tool to treat complex coronary lesions. With more experience and improved devices (i.e. coated wires, steerable microcatheters) the safety and efficacy of the procedures should be improved.
Introduction
The number of coronary interventions has been grown over the past years and the demand to treat complex lesions (e.g. very tortuous or very distal lesions, chronic occlusions) is raising. New tools and devices are therefore required.
So far, guide wire tips need to be pre-shaped to match the underlying vessel anatomy to cross the target lesion and to reach distal portions of the target vessel. Changing the shape of the tip during the procedure requires exchanging of the wire, thus making guide wire control sometimes difficult in complex anatomic circumstances. Also, during long and complex procedures the shape of the wire tip can get lost. Although wires with deflectable tips have been developed, their use has been limited. The magnetic navigation system represents a novel technology using magnetic fields to steer magnetic devices within the heart and the coronary vasculature. The system has been used successfully in electrophysiologic studies and catheter ablation1,2,3,4.
We hypothesize, that the magnetic navigation system can safely and effectively be used for the treatment of coronary stenoses. Therefore, the objective was to investigate the safety and feasibility of the magnetic navigation system in percutaneous coronary interventions (PCI).
Methods
The Niobe™-System
The principle of the underlying technique has been described in extension previously1,2. It consists of two computer controlled permanent magnets on each side of a fluoroscopy table (AXIOM Artis™, Siemens, Germany). The resulting uniform magnetic field (about 15 cm in diameter inside the patient’s chest) is 0.08 Tesla. As the two magnets are steerable in all degrees of freedom the resulting orientation of the magnetic field can be controlled in the same way. Small magnetic devices brought into the magnetic field will align according to their polarity like a compass needle. For coronary interventions a small magnet is installed at the guide wire tip. The orientation of the wire tip can now be controlled by changing the vector of the outer magnetic field. Advancing and retracting of the guide wire is to be done manually. The remaining steps of angioplasty (i.e. positioning the guiding catheter, balloon angioplasty and stent placement) are done in the conventional manner and do not require particular materials.
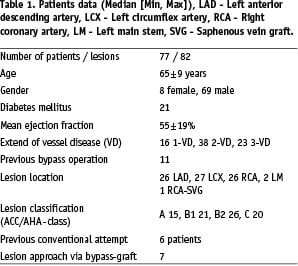
Control of the magnetic field can be done in different ways (Figure 1).
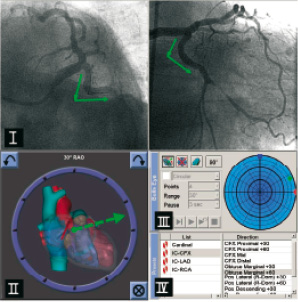
Figure 1. Ways of controlling the magnetic field: I) drawing vectors onto reference images, II) free control of the vector using a computer icon, III) using a bulls eye view, IV) using standard presets.
First, after taking two reference angiographic images (at least 45° different in angulation) of the target vessel the desired vectors can be drawn onto the images. The resulting vector is calculated by the computer. Second, the vector can be moved freely using a computer icon. Third, a “bullseye view” (with the wire tip in the center) can be used to modify the tip orientation even in very small steps. Fourth, a range of presets representing “standard” anatomic conditions is offered by the computer software. Once a vector is selected, positioning of the magnets will take less than five seconds. The guide wire is advanced (or retracted) manually stepwise distally to the culprit lesion. The flexibility of the wire tip is preserved during the procedure. After navigating the tip through the vessels curvatures using magnetic deflection it was also possible to turn off the magnetic field for passing the stenosis with the floppy tip, when the vector was not adequate. So the magnetic navigation technique can be combined with standard coronary wire technique.
Guide wires
Up to now there are two second generation guide wires available (Cronus™, Stereotaxis Inc., USA). Both are 0.014’’ in diameter, 180 or 210 cm in length and partially hydrophilic coated. They vary in the stiffness of the tip resulting in an intermediate and floppy grade. The shaft offers moderate support features. At the very tip of the coiled distal 2 cm of the wire a 3 mm - magnet (neodynium iron boron) is mounted.
Patients
Selected patients with (un~)stable angina and significant coronary stenoses or occlusions were treated with the magnetic navigation system. Patients with pacemakers or implantable defibrillators or acute myocardial infarctions were excluded. Informed consent form was signed prior to the procedure. This study was part of the initial safety and feasibility protocol approved by the ethical board of the Hamburg chamber of physicians.
Procedure
Vascular access was obtained via the femoral artery using 6 french sheaths. Diagnostic coronary angiography was done in the usual manner followed by biplane ventriculography. Prior to the angioplasty procedure patients received i.v. Heparin (70 I.U./kg), i.v. ASA (250 mg). Administration of GPIIbIIIa-receptor antagonists was left to the investigators discretion.
After positioning of the guiding catheter two reference images were taken and stored. The guide wire was stepwise moved forward using the magnetic field to direct the tip of the wire towards the distal part of the target vessel.
If attempts to cross the lesion failed, a switch to conventional wires (e.g. Graphix standard™, Boston Scientific Corporation or Cross IT™, ACS Guidant) was left to the investigators decision. Once the lesion had been passed the remaining procedure was made in the standard fashion (i.e. dilation and/or stent implantation).
Procedures were defined as successful if the lesions could be dilated with a residual stenosis of less than 30% (by visual estimation) and without flow limiting dissections.
Statistical analysis
Continuous variables are expressed as mean values ± standard deviation.
Results
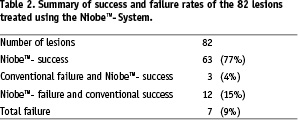
Eighty two coronary lesions in 77 patients were attempted to treat. Patient data is shown in table 1.
Ten lesions were total occlusions (6 older than 6 months). Seven lesions were approached via bypass-grafts (6 vein grafts, 1 left internal mammarian artery). In six patients prior unsuccessful attempts have been made with conventional angioplasty.
Mean fluoroscopy time was 13,9±8,4 min. Advancing the guide wire to the target lesion was successful in all cases. Target lesions could be crossed with the magnetic guide wire in 63 cases (77%). In 12 (15%) lesions switching from the magnetic tip wire to a conventional wire helped to cross successfully. Principally, the operator can advance the guidewire without directioning by the magnetic field, too. These failures using the magnetic wire were due to chronic total occlusion (2 lesions), severe calcification (5 lesions) and severe tortuosity with more than three 90° curves in the coronary vessel (5 lesions). Advancing a balloon was successful in 63 cases (77%), stents were implanted in 67 (82%) lesions including 15 drug eluting stents (22%). In 4 cases we could not place a stent over the magnetic wire. In 7 (9%) lesions total interventional failure was observed due to dissection type E/F (2/7) and unsuccessful recanalisation in chronic total occlusion (5/7). A summary is shown in Table 2.
In 3 (4%) cases magnetic wire navigation was successful in spite of prior interventional failure using conventional techique (example in Figure 2).
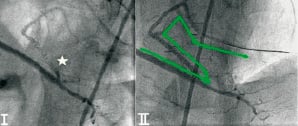
Figure 2. Subtotal stenosis (x) of the descending posterior artery proximal to the distal saphenous vein graft anastomosis (I). Previous attempts with conventional angioplasty failed. Using magnetic navigation (arrows) the guide wire could be advanced across the target lesion into the peripheral posterolateral branch. After dilation with 2 balloons (1.5 x 10 mm and 2.5 x 15 mm [Stormer™, Medtronic]) angiography showed only a mild residual stenosis with no significant dissection (II). Due to the sharp angle at the anastomosis site stents could not be advanced.
No vessel perforation or relevant pericardial effusion were observed. Five major dissections occurred: one after implantation of a stent, three in trying to cross subtotal lesions, one due to trauma of the guiding catheter to the left main stem. Four remained clinically non-significant or could be treated interventionally. However, despite immediate bypass surgery one patient died of hemodynamic failure due to a dissection of the complete left coronary artery during an attempted angioplasty of a complex lesion of the first left marginal branch.
Discussion
Precise guide wire control is an essential part for fastidious interventional procedures. We present the first data on magnetic guide wire control using the magnetic navigation system.
Since the first use of magnetic navigation in 19916 it has been published in neurosurgery7 and in electrophysiology studies of the heart1-4. The system has been developed from a biplane fluoroscopic imaging system with two electromagnets (0.15 Tesla, Telstar™, Stereotaxis Inc., USA) to a monoplane fluoroscopic system with two permanent magnets.
First experience
The present paper reports the results of treating the first coronary patients using the magnetic guide wire control in our hospital. 77% of the lesions could be treated successfully. We believe that this is at least partially related to the rather complex nature of the lesions (50% type B2 and C) including chronic total occlusion (11%) and prior interventional failure using conventional wire technique (7%). The low success rate of the magnetic navigation is most likely due to the patient selection. We rather included patients with at least moderate to complex vessel morphology and high grade stenosis. The patients were not included consecutively. With increasing experience (learning curve) and improved materials the success rate can be raised. In the beginning fluoroscopy was used to monitor wire tip movement leading to longer fluoroscopy times.
Guide wire control
The wire is advanced and retracted manually. There is no loss of the “tactile sensitivity” of the investigator. Motor drives for complete remote controlled procedures as in electrophysiology studies4 have not been used. As the curve of the wire tip is not pre-shaped compared to conventional wires, control of the wire without the magnetic field is very limited. With the magnets in navigate position, torquing of the wire (as often done with conventional systems) has no effect on the tip orientation as it is held in line with the magnetic field.
We think that this new technique is more applicable to difficult cases but this has to be shown. There is a potential advantage in deflecting the wire and than stretching the wire inside the vessel. This could be helpful e.g. for passing in-stent restenosis and reducing the via falsa under the struts. Also deviation into sidebranches could be avoided more easily.
Due to the construction of the wire with the magnet at the end, the tip itself may be too large and blunt in profile and not flexible enough to cross long occlusions or severely calcified lesions.
Crossing the lesion is one but essential part of angioplasty. However, advancing balloons and stents into complex lesions often remains the critical part of the procedure. As the wires so far offer moderate support features, new wires and even new devices (e.g. steerable microcatheters) are in preparation. A complete remote maneuver for PCI similar to the usage in electrophysiology would have the potential to reduce fluoroscopy exposure for the operator, but it was not tested so far.
The magnetic navigation system has certain limitations mainly due to the close position of the magnets on each side of the patients table. Lateral angulation of the C-arm is limited within a range of 30° towards each side leading to sometimes non-optimal view inside stenotic areas and superimposed structures (i.e. spine) especially in left angulated views.
Limitations
This study was designed to proof the feasibility of magnetic navigation in coronary interventions. As there is no control group, a comparison between magnetic assisted and conventional angioplasty is not possible.
Conclusion
Magnetic guidance of the guide wire during coronary interventions is feasible and a promising tool to treat coronary lesions. However, more experience and different types of guide wires with improved features (e.g. extra support) are needed. Additional devices are in preparation to proof equality or even superiority over conventional angioplasty.
Acknowledgement
This study was performed with the generous support of Siemens Medical Solutions, Germany and Stereotaxis Inc., USA.
