Abstract
Aims: As part of the EAPCI Young Initiative, the European Association of Percutaneous Cardiovascular Interventions (EAPCI) conducted a survey to address the educational needs of young interventional cardiologists.
Methods and results: A questionnaire was distributed to all individuals registered in the ESC database aged <36 years with an interest in interventional cardiology. Nearly two-thirds of participants (60%) indicated that they had difficulty in finding a fellowship training position. The desire for a fellow’s course at European level was expressed by 95%, while 94% were in favour of developing a network of young interventional cardiologists in Europe. More than three-quarters of respondents (79%) said they had had difficulty in obtaining funding to attend EuroPCR. Multiple difficulties were identified in setting up a research programme, two of the more frequent being problematic access to research networks and the difficulties of finding a mentor. Career orientation was identified as another issue, with more than half of respondents (59%) declaring they followed career options by chance.
Conclusions: The survey underlines the need to fill a gap in order to address the needs of young interventional cardiologists. It may serve as a starting point for developing educational initiatives targeted at young interventional cardiologists.
Introduction
Young interventional cardiologists constitute the future workforce and leadership in the field of interventional cardiology. At the beginning of a professional career, young interventional cardiologists have specific needs in terms of education and career orientation. However, there is no clear perception about the unmet needs of this professional group. In order to elucidate and address these concerns, the European Association of Percutaneous Cardiovascular Interventions (EAPCI), a registered branch of the European Society of Cardiology (ESC), last year appointed young interventional cardiologists to establish the “New Initiatives For Young Interventionalists” (NIFYI) committee1. The NIFYI committee recently conducted a survey to obtain information on the educational and training needs of young cardiologists (arbitrarily defined as age <36 years) with an interest in interventional cardiology. The results of this survey are presented here.
Methods
The ESC database comprises 293,932 individuals, but only 178,884 have provided their birthdate. Among these, 42,748 (24%) were <36 years old, and 6,660 (16%) were both <36 years old and had expressed their interest in interventional cardiology. However, only 4,619 provided their email address and this sample constitutes the study population.
The Young Survey was e-mailed to those 4,619 individuals on the 28th January, 2013. A reminder was sent on the 8th February, 2013, to individuals who did not respond to the first e-mail.
The survey comprised questions on training and education, research, networking and communication, and professional issues. Questions were proposed by the EAPCI committee “New Initiatives For Young Interventionalists” and validated by the EAPCI president and the president elect. The survey included multiple choice questions (MCQs), for which the results are aggregated below, as well as open questions. It was not mandatory to reply to the entire questionnaire.
Of the 4,619 questionnaires sent on 28th January, 4,471 were delivered. The e-mail was opened by 1,128 individuals (24%), and 145 (3.1%) clicked the survey link. Of the 3,365 reminders sent on 8th February, 3,357 were delivered, 328 (9.7%) were opened and 43 (1.3%) were clicked.
Results
DESCRIPTION OF THE RESPONDENTS
A total of 188 individuals clicked the survey link, but only 148 answered the survey. Among them, 111 individuals (75%) worked in the field of interventional cardiology. Only the latter group had access to the remainder of the questionnaire. Of the 111 relevant respondents, 106 people responded to questions about their role, gender, age and geographical location. Of these, 30 (28.3%) were interventional cardiologists, 75 (70.8%) were interventional cardiologists in training and one person was a technician. There were 84 replies from males (79.2%) and 22 from females (20.8%). The age distribution was as follows: 20 were <28 years (19%), 22 were 28-30 years (21%), 23 were 30-32 years (22%) and 41 were >32 years of age (39%).
Europe was the primary continent of origin with 72 (68%) respondents, followed by Asia with 16 respondents (15%), Africa with 13 respondents (12%), and America with 5 responses (5%). The country with the greatest number of respondents was Spain (11), followed by Egypt (10), Italy (9), Turkey (7) and Romania (5).
FINDING A FELLOWSHIP
There were 105 replies to the question, “Did you/do you have difficulties in finding a fellowship in interventional cardiology?”. Of these, 63 respondents (60%) said yes and 42 (40%) said no (Figure 1). Respondents <31 years of age were more likely to reply yes to this question (69.1%) than no (30.9%), while the answers of those >32 years of age were mixed (49.0% yes, 51.0% no).
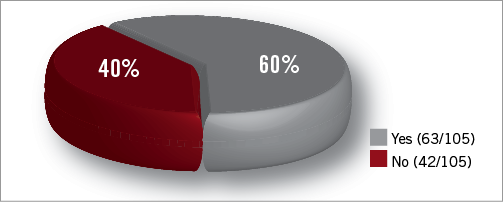
Figure 1. Did you/do you have difficulties in finding a fellowship in interventional cardiology?
When asked why they had/have difficulties, there were 62 responses. From a list of choices, financial issues were cited most frequently (40 respondents; 65%), followed by networking issues (29 respondents; 47%), insufficient awareness of high quality fellowship programmes (23 respondents; 37%) and national regulations (17 respondents; 27%).
The age split is detailed in Figure 2. Networking issues was the top reason cited by both age groups.
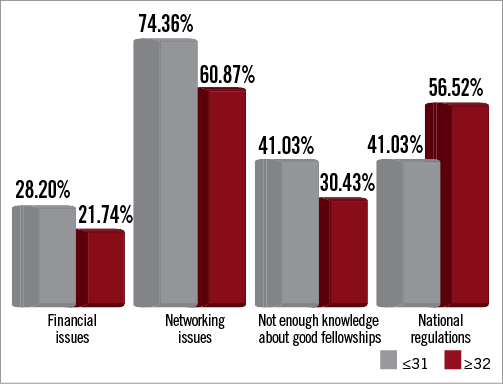
Figure 2. Why did you have difficulties in finding a fellowship? Distribution by age.
There were nine open replies to the question about why they had/have difficulties in finding a fellowship in interventional cardiology. Reasons included family and personal issues, not enough opportunities, techniques unavailable, lack of experienced cardiologists and working obligations.
INTERNATIONAL FELLOWS’ COURSE AT EUROPEAN LEVEL
There were 61 replies to the question “Do you think that there is a need for a fellows’ course at a European level?”. Of these, 58 respondents (95%) indicated yes and 3 (4.1%) said no (Figure 3). The response was overwhelmingly yes in both age categories: 97.4% of respondents aged <31 years and 90.9% of respondents aged >32 years replied yes.
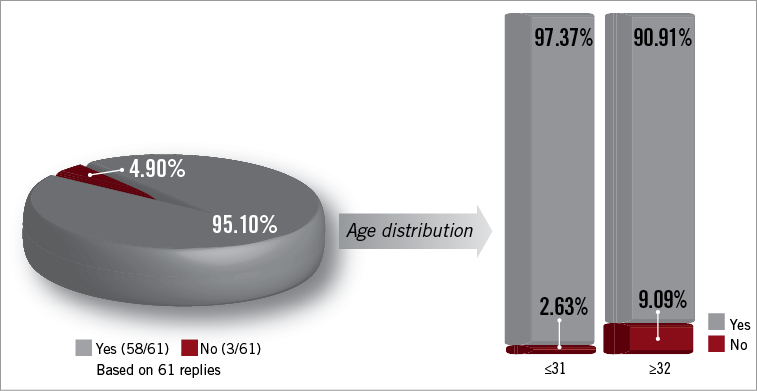
Figure 3. Do you think there is a need for a fellows’ course at a European level?
When asked, “Which particular topic(s) would you like to be addressed in this course?”, the most popular answer from a list of choices was technical focus, which was chosen by 51 respondents (88%). It was followed by strategy/decision-making process (49 respondents; 85%), how to extrapolate data from clinical trials to a particular patient (30 respondents; 52%), and global patient appraisal (13 respondents; 23%).
Age repartition is detailed in Figure 4. Briefly, technical focus was the main choice of topics for respondents aged <31 years, with 89%, whereas for respondents aged >32 years the most popular topic was strategy/decision-making process (86%).
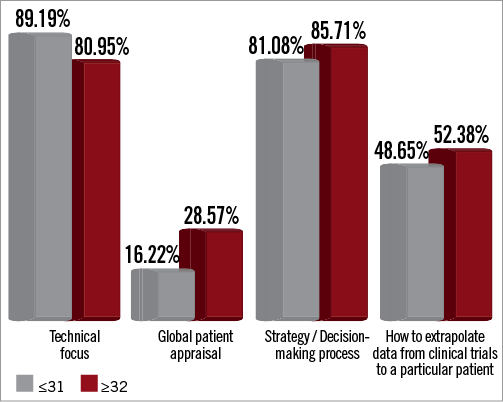
Figure 4. Which particular topic(s) would you like to be addressed during a European fellows’ course? Repartition by age.
There were 27 open replies to the question, “What do you expect from a fellows’ course at a European level?” Responses included better education, acquire improved knowledge, obtain new ideas, easier accessibility to training opportunities, get more experience, strategy, quality, understand the decision-making process, standardisation, transfer knowledge to colleagues, apply it to patients, discover new technologies and devices, and have access to centralised information on training centres.
EUROPCR
There were 98 replies to the question, “Do you encounter difficulties being invited to EuroPCR?”, with 77 people (79%) saying yes and 21 (21%) saying no (Figure 5). Difficulties were encountered by the vast majority of respondents in both age categories: 81% of <31s and 77% of >32s said yes.
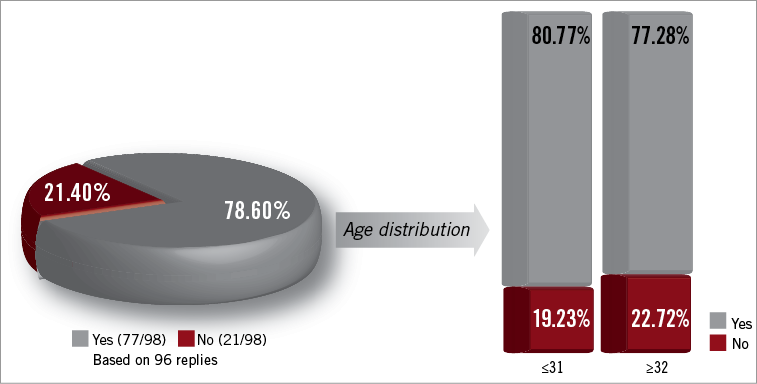
Figure 5. Do you encounter difficulties being invited to EuroPCR?
The idea of interactive sessions by and for young interventional cardiologists was popular, with 95 respondents (97%) answering yes to the question, “Would you be interested in 5 interactive sessions designed by and for young interventionists?”, and just 3 (3%) replying no. People in both age categories strongly supported the idea, with 98.1% of <31s and 95.5% of >32s replying yes to the question.
There were 97 replies to the question, “Which particular topic(s) would you like to see incorporated in these sessions?”. The most popular answer from a list of choices was “PCI: planning your strategy”, which was chosen by 73 people (75%). This was followed by technical aspects of PCI (70 respondents; 72%), FFR/intracoronary imaging (55 respondents; 57%), structural/valvular heart disease (46 respondents; 47%), global patient appraisal (21 respondents; 22%) and peripheral artery disease (21 respondents; 22%).
Age repartition is represented in Figure 6. For respondents aged <31 years, the most popular topic was “PCI: planning your strategy”, which was chosen by 81% of respondents in this age category. For this group the next most frequent choice was technical aspects of PCI (77%), followed by FFR/intracoronary imaging (64%), structural/valvular heart disease (48%), peripheral artery disease (21%) and global patient appraisal (19%).
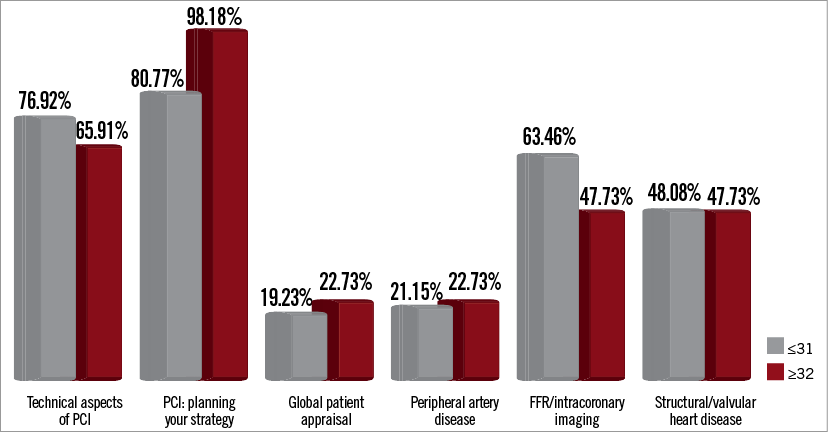
Figure 6. Which particular topic would you like to be addressed during interactive sessions “by and for” young interventionists during EuroPCR? Repartition by age.
Nearly all (98%) respondents aged >32 years indicated they would like the topic “PCI: planning your strategy” incorporated in the sessions. The next most common choice was technical aspects of PCI (66%). This was followed by FFR/intracoronary imaging and structural/valvular heart disease (both chosen by 48% of >32s), and global patient appraisal and peripheral artery disease (both chosen by 23% of >32s).
WEB-BASED LEARNING TOOL
There were 98 replies to the question, “Are you interested in a web-based learning tool?”, with 93 (95%) saying yes and 5 (5%) responding no.
RESEARCH
There were 97 replies to the question “What most prevents you setting up your own research programme?”. The most frequent answer from a list of choices was access to people networks to be involved in research (chosen by 43% of respondents). This was followed by difficulties in finding a mentor (42%), working in non-academic centres where research facilities are scarce (40%), lack of time (35%) and knowledge of the basics of research (30%) (Figure 7).
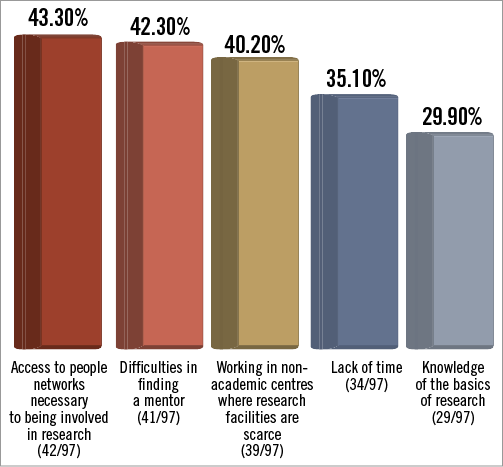
Figure 7. What most prevents you setting up your own research programme?
There were 12 open replies to the question, which included fixed-term employment (max. six months), support, collaboration, lack of funding, and no research unit.
NETWORKING
There were 97 responses to the question, “Would you be interested in developing a network of young interventional cardiologists in Europe?”, with 91 respondents (94%) saying yes and six (6%) responding no.
When asked, “Which kind of network would you be interested in?”, the top choice from a list of options was Facebook (58 respondents; 64%). This was followed by LinkedIn (33 respondents; 36.3%) and Twitter (13 respondents; 14.3%).
There were 48 open replies to the question, “What do you expect from this network?”. Responses included discussion, support, find fellowships, collaboration, access new technologies, improvement, share experiences and ideas, networking, communication, brainstorming, community of practice, participate in studies, cooperation, standardisation, interaction, and know-how.
CAREER AND ORIENTATION
There were 97 replies to the question, “What are the primary difficulties in defining your career and navigating the options?”. The most frequent answer from a list of choices was “you actually don’t know the options, you learn them by chance” (57 respondents; 59%). This was followed by “advantages and pitfalls of academic and non-academic careers are unclear” (41 respondents; 42%), and “your outlook is local, you don’t aspire to a more European dimension and don’t take mobility into account” (32 respondents; 33%) (Figure 8).
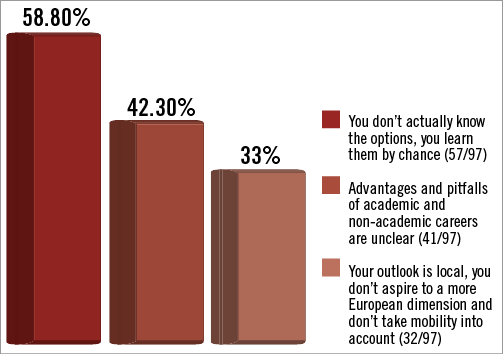
Figure 8. What are the primary difficulties in defining your career and navigating the options?
There were 10 open replies to the question, which included: programme and mentor needed, not always transparent, spend some years abroad, find a position as interventional cardiology assistant, no meritocracy, and no studies recognition abroad.
Discussion
The term “young interventional cardiologist” covers a broad range of experience from the resident in cardiology interested in becoming an interventional cardiology fellow to the young cardiologist beginning their professional career as an independent practitioner. These individuals are at stages in their career mostly dependent on education and experience, while a great part of their education is not centred on their needs. The “Young Survey” identifies these unmet needs in more detail. For the majority of questions there was an overwhelming majority in the responses. Some strong messages have been sent to the community by young interventional cardiologists through this survey.
Nearly two-thirds of respondents (60%) indicated difficulties in finding a fellowship programme. Conversely, many institutions encounter difficulties in finding appropriate fellows with an interest in interventional cardiology. In order to facilitate contact between training programmes and young cardiologists with an interest in interventional cardiology, the NIFYI Committee has created a web-based database of training centres welcoming fellows across Europe called “CathGo”, which was launched during EuroPCR 2013. CathGo has been assembled to serve as a reference tool for young interventional cardiologists looking for training opportunities across European countries, to add visibility to centres willing to accept fellows from abroad and, ultimately, to help rationalise the flow of young interventional cardiology fellows throughout Europe. The CathGo search engine is hosted in the ESC website: www.escardio.org/communities/EAPCI/younginterventionalists/Pages/cathgo.aspx
An overwhelming 95% of respondents expressed their desire for a fellows’ course at a European level. An annual fellows’ course in Krakow is currently endorsed by the EAPCI. In view of the survey results, this course probably needs to be further developed to move from a regional to a true European fellows’ course involving every fellow working in the countries affiliated to the EAPCI.
Overall, more than three-quarters of respondents (79%) indicated difficulties in obtaining funding to attend EuroPCR. This is a very important issue as young interventional cardiologists theoretically benefit most from education. As the leading congress for interventional cardiology education, EuroPCR should be attended by the majority of young interventional cardiologists. Specific sessions have been developed for this purpose, and this survey confirms the attractiveness of those sessions. The possibility to offer grants or sponsorship to young interventionists to attend EuroPCR has to be further explored.
An interest in a web-based learning tool was described by 95% of the respondents. The ESC eLearning platform (ESCeL) in interventional cardiology was launched in February 2013. It aims to provide the highest standards of training and education at the lowest possible cost to as many cardiology trainees as possible. The principle is to homogenise training throughout Europe so cardiologists have access to the same high quality education regardless of origin. Such standardisation of training has been made even more important by the recent EU directives on free movement of patients and healthcare professionals across European borders, expected to be introduced in 2014. The EAPCI programme built around the EAPCI Core Curriculum and PCR-EAPCI Textbook provides a certificate of excellence in training in interventional cardiology. It has been designed to last 24 months maximum and consists of three modules: Knowledge, Skills and Professional development (which is optional).
Research is an important aspect of our specialty. However, respondents faced numerous difficulties in setting up a research programme, with more than 40% citing difficulties in access to people networks, finding a mentor, and working in non-academic centres where research facilities are scarce. Europe has many centres of excellence that offer research training. More information about the possibilities may help young interventional cardiologists to identify optimal opportunities. Every year, thanks to the financial support of industry partners through an educational grant, the EAPCI offers grants for one year of research or training fellowships in an ESC member country other than the candidate’s country of residence. The ultimate goal is to enable young candidates to enhance academic standards as well as encourage exchanges and interactions from country to country.
A large proportion (94%) wanted to develop a network of young interventional cardiologists in Europe. We all know that networking is important in our activities. Young interventional cardiologists expressed the need to develop networking using web-based networks. The development of such a network is a real challenge for the NIFYI committee. The ideal platform has still to be discussed. It is important to note that ESCeL V2.0 will offer the possibility of networking.
Finally, career orientation is difficult at any point in life, but is crucial at the beginning since it may have an important impact on future directions. However, this is also a period when the different options may appear confusing. The answers to the survey expressed this point very clearly. More than half of respondents (59%) declared that they had discovered career options by chance, while 42% said that the advantages and pitfalls of academic and non-academic careers were unclear.
Limitations
This survey presents some limitations. The first one is that only a small percentage of people replied. Therefore, the results are not necessarily representative of the whole young interventional cardiology community. However, for the first time within EAPCI, this survey represents a structured approach to shed light on the unexplored issue of the expectations and unmet needs of the young generation. The second limitation is that MCQs, although allowing answer aggregation, are directive by nature in that they propose all possible responses. For that reason, the possibility of adding open replies was left to the respondents.
Conclusions
EAPCI believes that young interventionalists are a key target for education because they represent the future pillar of the specialty. This survey reveals a large discrepancy between educational offers and the unmet needs of young interventional cardiologists. The EAPCI in general, and the NIFYI committee in particular, will begin to fill the gaps between the educational needs of young interventional cardiologists and existing material. The continuous strive to advance knowledge, education and quality of care will ensure the longevity and quality of EAPCI’s future membership.
Conflict of interest statement
The authors have no conflicts of interest to declare.
