Introduction
Cardiac catheterisation was introduced in 1929 when the German physician Werner Forssmann inserted a plastic tube in his cubital vein and guided it to the right chamber of the heart. In 1960 F. Mason Sones, a paediatric cardiologist, accidentally injected radiocontrast in a right coronary artery instead of the aortic root. He developed the procedure further, and is credited today with the discovery of selective coronary angiography.
Use of invasive angiography today
Today, invasive angiography is used for two main purposes in interventional cardiovascular medicine:
a) To establish a diagnosis of cardiovascular disease e.g., coronary and peripheral atherosclerosis, myocardial infarction, pulmonary embolism, aortic dissection, or vascular malformations etc.
b) To guide and to plan percutaneous interventions e.g., coronary stent implantation, percutaneous valve repair, or the occlusion of a persistent foramen ovale etc.
For both purposes radiation is used in two ways:
a) As plain x-ray to indicate the position of interventional tools in relation to anatomic landmarks, or to demonstrate the presence of cardiovascular calcifications or of implanted prosthetic material.
b) As angiography, combining x-ray with the selective or semi-selective application of radiocontrast to show the mould of anatomical structures in real time which also allows assessing their physiology and function.
Choosing the appropriate angiographic view
The problem of the diagnostic and therapeutic use of angiography is the mandatory translational process required to be executed by the operator from the acquired two-dimensional image to the three-dimensional target.
To address this problem successfully a detailed anatomical knowledge is mandatory. An appropriate imaging technique is also obligatory using different angiographic views to realistically picture the target region with no, or very little bias caused by the image acquisition.
In particular in complex anatomical structures such as for example the coronary artery tree, complete visualisation requires care and rigour to ensure complete anatomical documentation. Often bifurcations and vessel foreshortening and overlap cause errors in stenosis estimation.
Generally, for left anterior descending artery (LAD) and LAD/diagonal bifurcation visualisation the cranial views are most useful (Figure 1).
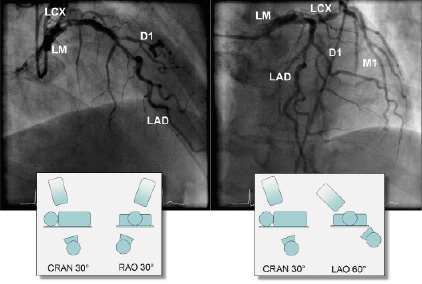
Figure 1. Cranial views of the left coronary artery. LM: left main; LAD: left anterior descending; LCX: left circumflex; D1: first diagonal; M1: first marginal; LAO: left anterior oblique; RAO: right anterior oblique; CRAN: cranial
For circumflex and proximal epicardial visualisation the caudal views are most useful (Figure 2).
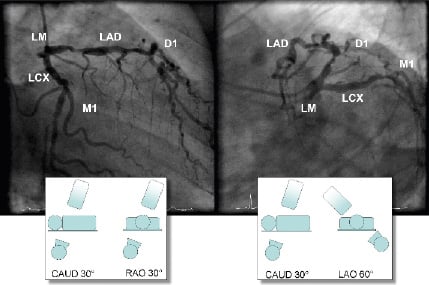
Figure 2. Caudal views of the left coronary artery. LM: left main; LAD: left anterior descending; LCX: left circumflex; D1: first diagonal; M1: first marginal; LAO: left anterior oblique; RAO: right anterior oblique; CAUD: caudal
Initial angiographic imaging of the right coronary artery (RCA) in the left anterior oblique (LAO) position provides optimal view on the ostial and proximal segments of the RCA. The bifurcation of the distal RCA is best seen in a LAO/cranial position (Figure 3).
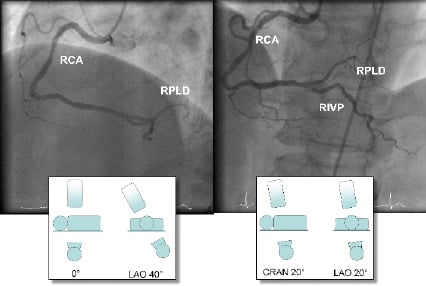
Figure 3. LAO views of the right coronary artery. RCA; right coronary artery; RPLD: R. posterolateral dexter; RIVP: R. interventricular posterior; LAO: left anterior oblique; CRAN: cranial
Other techniques such as the left ventriculogram have become of less interest with the advancement of non-invasive imaging. However, besides the possibility for haemodynamic measurements, the visualisation of the left ventricle using radiocontrast remains an important aspect of a complete angiographic study. The two standard views for ventriculography are the RAO projection which demonstrates the anterior, apical and inferior ventricular wall. A LAO view allows for better imaging of the lateral and septal ventricular wall (Figure 4).
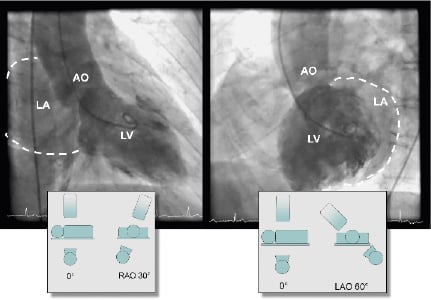
Figure 4. Standard views of the left ventricle. LV: left ventricle; LA: left atrium; AO: aorta; LAO: left anterior oblique; RAO: right anterior oblique
Aspects covered in the online version of this chapter
The online version of this chapter of “Tools & Techniques” will give practical advice for the choice of the appropriate angiographic view for diagnosis and percutaneous treatment of cardiovascular disease with particular emphasis on coronary artery disease. Other aspects that will be covered are radiation protection for patients and operators and the protection of renal function by minimising the use of radiocontrast.
