Abstract
Aims: Interventional cardiologists are amongst the most intensive radiation users within medicine. To assess the implications of this usage, the “Women In Innovation” Group (WIN) created a web-based survey called “WIN for Safety” distributed through the European Association of Percutaneous Coronary Intervention (EAPCI) to all catheterisation laboratory healthcare professionals, enquiring about radiation protection measures, compliance with monitoring, health (orthopaedic issues), radiation-associated problems (cataracts and cancer) and restrictions imposed upon the pregnant female.
Methods and results: In total, there were 615 participants: 72.8% were interventional cardiologists. Most (73.5%) of them were male and 63.3% were aged 31-50 years. A radiation collar badge was used by the majority (64.4%) and the most frequently utilised protective measure was the thyroid shield (87.2%). Potential illnesses related to radiation exposure included 19.5% orthopaedic problems (back/neck/hip pain), 5.5% varicose veins, 2.4% blood count problems and 2.0% cataracts. Notably, an association between orthopaedic problems and years of exposure was found (p=0.001). Overall, only 2.2% had ever been diagnosed with a cancer, with a trend for more females to be affected (4.4% vs. 1.8%; p=0.067). Finally, 62.1% have restrictions imposed upon the pregnant female in the working environment.
Conclusions: Awareness of radiation in the field of interventional cardiology is essential. The main risk is orthopaedic problems and measures should be taken for prevention. Cancer has not been demonstrated to be a direct consequence; however, we should remain vigilant and monitor individuals.
Introduction
There are several occupational hazards for individuals who have chosen interventional cardiology as a career. The major concern is that of radiation exposure, with interventional cardiologists amongst the most intensive radiation users within the medical profession.1-3 This has been theoretically correlated with a higher risk of developing malignancy.4 The prevalence of cancer amongst interventional cardiologists remains to be clarified and it is consequently unclear whether this poses a significant occupational hazard. Importantly, radiation protection measures can lead to an overall reduction in the dose obtained by the individual; however, this entails wearing heavy lead aprons and collars. Such apparel can lead to the development of orthopaedic problems, with a significant proportion of interventional cardiologists suffering from back and neck pain.1,5-9 As a further issue, there remains a debate concerning female workers in the cardiac catheterisation laboratory throughout pregnancy; indeed radiation issues may prevent women from pursuing such a career.
An initial pilot study, performed through the Society for Cardiovascular Angiography and Interventions (SCAI) by the Women in Innovations (WIN) group, consisting of 122 cardiac catheterisation laboratory workers (68.0% interventional cardiologists), demonstrated mechanical back and neck problems in 78.6%. The aim of this “WIN for Safety” survey was to enable attitudes towards radiation exposure and health to be explored, including restrictions upon the pregnant female radiation worker.
Methods
An anonymous web-based survey was developed by members of the WIN group (www.winforsafety.com) and the Centre of European Cardiovascular Research (CERC), Massy, France and was distributed to all 3,994 European Association of Percutaneous Coronary Intervention (EAPCI) members via an e-mail. This was subsequently distributed to all workers within cardiac catheterisation laboratories in Europe, including interventional cardiologists, technicians, nursing and auxiliary staff. The questions were formatted so that responses were either yes/no or check boxes. In the case that more information was required, write in responses were included.
The survey identified baseline characteristics including age, gender, country, profession and number of years of exposure to ionising radiation. In addition, the use of radiation protection measures, including thyroid collars, lead glasses and leg shields were explored and the compliance with radiation monitoring. Health questions focussed on orthopaedic problems (back, neck, hips) and problems associated with chronic radiation exposure (questions regarding history of cataracts as well as any type of cancer). In addition, the health concerns of the individuals regarding radiation exposure were enquired about. Finally, participants were questioned about the practices of pregnant women in the cardiac catheterisation laboratory and any restrictions imposed upon them.
The results were reported as descriptive statistics and chi-square analysis for discrete variables. Statistical analysis was performed with the Statistical Package for Social Sciences Version 18.0 (SPSS Inc., Chicago, IL, USA). A p-value of <0.05 was considered statistically significant.
Results
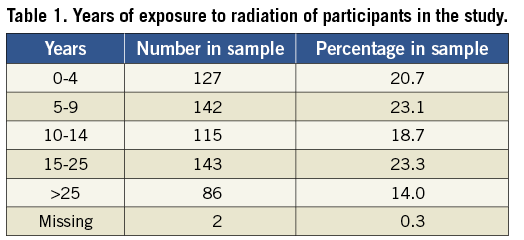
In total, 615 cardiac catheterisation workers completed the online survey (a response rate of 15.4% if we consider that 3,994 are EAPCI members). Of these, 73.5% were male with a wide spread in the age groups (Figure 1). The most frequent profession was that of interventional cardiologist (72.8%), followed by nursing staff (9.4%), radiography technician (8.0%), interventional radiologist (4.6%) and other (3.9%). The participants came from throughout Europe, with France (18.7%), Spain (11.4%), the Russian Federation (10.7%) and Italy (10.2%) comprising the majority (Figure 2). The sample contained a broad distribution of respondents in terms of years exposed to interventional procedures (Table 1).
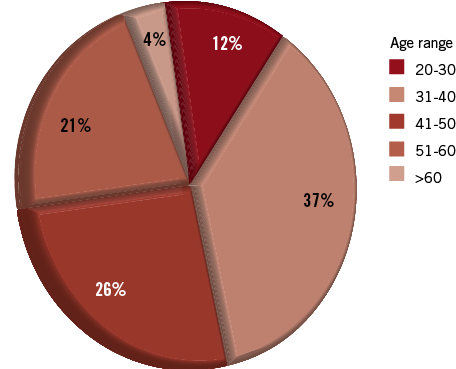
Figure 1. A pie chart to illustrate the varying age groups of participants in our study.
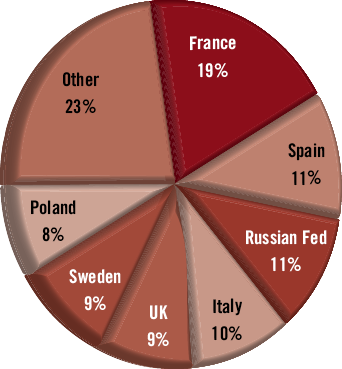
Figure 2. A pie chart demonstrating the countries of residence of study participants.
RADIATION PROTECTION
With regard to radiation monitoring, the majority of individuals acknowledged always wearing a radiation collar badge (64.4%), with 17.7% wearing the badge most of the time, 6.5% some of the time and 4.1% occasionally. Of note, 7.0% of respondents admitted to never wearing a radiation collar badge for monitoring purposes. Overall, 65.9% of individuals reported that they reviewed regularly the radiation exposure data. Of those who did, most did this monthly (50.9%) or quarterly (33.8%) (Figure 3). Only 6.8% of individuals questioned had been stopped from working in the lab due to excessive radiation exposure. Interestingly, 10.6% of respondents had actually stopped working in the lab themselves due to personal concerns regarding the exposure to radiation.
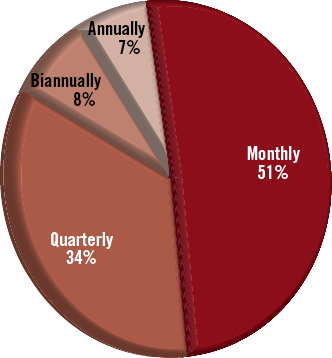
Figure 3. An illustration of how frequently participants in our study review their personal radiation exposure data.
Figure 4 demonstrates the use of radiation protection measures by the individuals completing the survey. The most frequently utilised was the thyroid shield with 87.2% always wearing this during procedures.
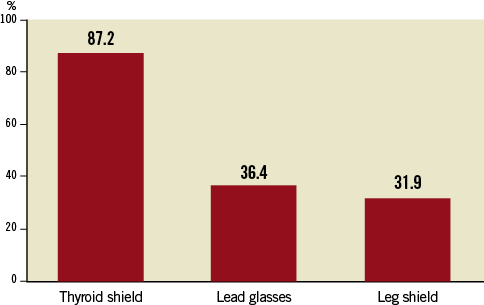
Figure 4. Use of radiation protection measures by the individuals completing the survey.
HEALTH CONCERNS
The majority of people (62.9%) actually had no health concerns regarding the occupational exposure to radiation. Of those who did report a concern, 8.6% worried about developing cataracts, 8.3% about cancer, and 2.1% about abnormalities in their blood count.
Potential illnesses related to radiation exposure, which were reported by respondents, included 19.5% with orthopaedic problems (back/neck/hip pain), 5.5% with varicose veins, 2.4% with problems with the blood count and 2.0% with diagnosed cataracts. Figure 5 demonstrates the incidence of radiation associated illnesses according to the years of exposure to radiation. Notably, an association between orthopaedic problems and years of exposure was found (p=0.001) in addition to the occurrence of varicose veins (p=0.046). The diagnosis of cataracts did not depend on the years of exposure to radiation (p=0.914).
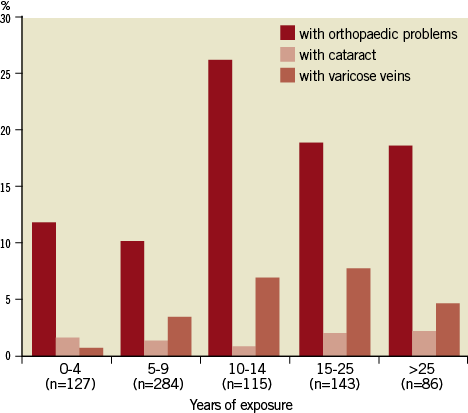
Figure 5. A graph to illustrate how the years of exposure to radiation are correlated with the incidence of medical conditions.
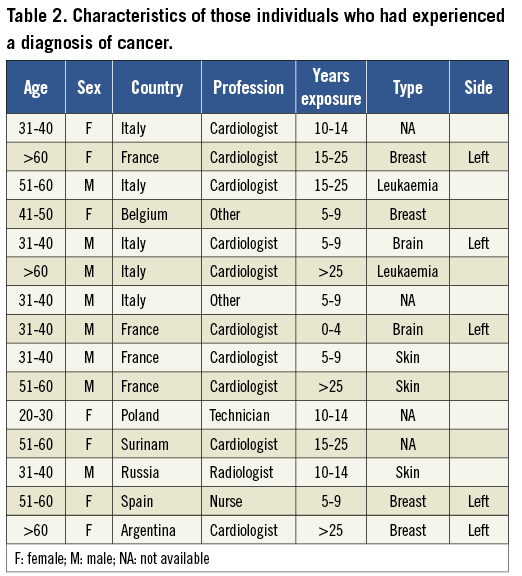
Overall, only 2.2% had ever been diagnosed with a cancer. The details of these diagnoses and the characteristics of the individuals are displayed in Table 2. Interestingly, there was a trend for more females to have been previously diagnosed with cancer in this study (4.4% vs. 1.8%; p=0.067).
PREGNANCY ISSUES
In total, 62.1% reported that restrictions were imposed on pregnant workers in their working environment. A minority of participants (20.2%) reported that pregnant females could continue to work in the cardiac catheterisation laboratory in their institution.
Discussion
The main findings of the WIN for Safety survey are: 1) The majority of individuals working in the cardiac catheterisation laboratory are aware of the need to monitor radiation exposure and utilise available protection methods; 2) The most common medical condition related to exposure to radiation was an orthopaedic problem; 3) The years of exposure to radiation had an impact upon the occurrence of orthopaedic problems, as well as the incidence of varicose veins; 4) A diagnosis of cancer was made in 2.2% of individuals, with a trend for this to be more common in the female radiation worker; 5) Measures are in place in the majority of institutions to protect the pregnant female radiation worker.
The field of interventional cardiology poses distinct occupational hazards to cardiac catheterisation laboratory workers.5-7,10-12 The recent advances within this discipline have led to the treatment of more complex disease, including the advent of percutaneous valvular therapies,13 with subsequent lengthy procedures and high radiation volumes. Therefore, the major concern is that of radiation exposure and the potential risk of cancer development.4 It is essential to measure radiation levels and the majority of radiation workers do wear radiation collar badges. However despite this being mandatory within Europe, this is not strictly adhered to (53.0% in France and 85.7% in Italy, respectively).
It is reassuring to know that the majority of individuals in our survey are fully aware of the potential risks associated with radiation exposure and take adequate protection measures. However, as a likely consequence of wearing a lead apron, the most frequent health problem in our survey was that of orthopaedic discomfort. It has been previously described that wearing lead aprons for many hours, may result in orthopaedic problems.1,5-9 In fact, compared with orthopaedic surgeons who occasionally wear a lead apron and rheumatologists who never wear a lead apron, invasive cardiologists have a greater incidence of spine problems, previously labelled as “interventionalist’s disc disease”.6
In 2004, SCAI conducted a Web-based survey of occupational health problems in 424 interventional cardiologists with 42% of responders reporting spine (lumbosacral and cervical) problems.5 Moreover, in the subsequent survey by the WIN group through SCAI, mechanical back and neck problems were reported in 78.6% of the participants (n=122). Interestingly, in our European survey, which is to the best of our knowledge the largest conducted, only 19.5% of the participants reported back, neck or hip problems. We cannot exclude that such a finding could be the result of improvements in the ergonomic design of radiation protection apparel, which have become more lightweight and generally consist of two pieces, which may distribute the weight of the protection more evenly. In addition, our study included all healthcare providers (not only high volume physicians) as compared to the survey conducted in 2004 by SCAI that included only interventional cardiologists who performed a high number of procedures. It must also be considered that there is a relatively high incidence of back problems in the general population, ranging from 5.6% to in excess of 30.0%.14-16 Notably, in our survey, the length of time working in a radiation environment was correlated with orthopaedic problems. Therefore adequate preventative measures are essential to try to further reduce the incidence of orthopaedic problems, as these have been demonstrated to increase sick leave, the need for surgery and even curtail careers.5 Hospital employers should be aware of the possible effects from radiation protection and preventive measures for orthopaedic problems such as proper posture during work and weight control, as well as exercise should be taken by the employee.
In addition to orthopaedic problems, another condition correlated with radiation exposure was that of varicose veins, which occurred in 5.5% of individuals.17 However, the incidence in our study appeared low, as up to 40% of men and 32% of women over the age of 18 years suffer from varicose veins.18
Conversely with the use of other radiation protection measures, lead glasses were used by only 36.4% of participants in our survey, which is low and should be improved. In our study, the incidence of cataracts was relatively low (2.0%) and cumulative exposure to radiation did not appear to be a risk. Nonetheless, it has been well described that the eye is particularly sensitive to radiation exposure and prone to radiation-induced cataracts.19,20 Moreover, it has been demonstrated that there is a significant increase in radiation-associated lens changes in cardiac radiation workers compared to controls (38% vs. 12%; p<0.005).20 The ongoing “Occupational Cataracts and Lens Opacities in Interventional Cardiology” (O’CLOC) epidemiological study, is evaluating the rate of cataracts and lens opacities in matched groups of invasive and non-invasive cardiologists.21 Protection measures in the form of lead glasses are available and certainly should be encouraged to prevent the possibility of cataract and visual deterioration. One of the reasons for the low usage may be due to the fact that lead glasses are expensive and this could be addressed by the employer.
Of note, cancer only occurred in 2.2% of the respondents of this survey. Population-based analysis has estimated an incidence of 286.9 cases of cancer per 100,000 people in the age range 45-49 years in the European population,22 which is lower than in this study. However, there has been no clear correlation between occupational radiation exposure and the development of cancer, only a suggestion that fluoroscopically-guided procedures are linked to it.8,23 A study has demonstrated that interventional cardiologists working in high-volume catheterisation laboratories have higher levels of somatic DNA damage when compared with clinical cardiologists.24 A further recent study has evaluated the incidence of brain tumours in six interventional cardiologists and three interventional radiologists. The study concluded that this may be a chance occurrence but occupational radiation exposure is biologically plausible.25
Interestingly there was a trend for more cancer diagnoses in the female radiation worker, (4.4% vs. 1.8%; p=0.067), with the majority of cases in the female being breast cancer. It has previously been described that females are 38% more sensitive to cancer damage for any given radiation exposure.26 Certainly breast tissue is very sensitive to radiation exposure and cumulative exposure may well increase the risk.27 Indeed, a study of 56,436 female radiology technicians revealed 1,050 cases of breast cancer and concluded that daily low dose radiation exposure over several years may increase breast cancer risk.28 Often, lead aprons do not provide adequate cover of the axillary tissue area, especially if they are not fitted correctly. It is possible to have a lead apron with sleeves, which ensures full coverage of this area, in addition to dedicated breast shields. The use of these items should become mandatory for the female interventional cardiologist who performs many procedures to aim to potentially reduce the risk of breast cancer.
Due to many confounding factors, it is difficult to demonstrate a direct correlation between radiation exposure and cancer. However adequate radiation protection measures must be used and the effects of radiation in interventional cardiology can only be detected by long-term follow-up on large cohorts. Dedicated registries using matched control groups are therefore necessary
Finally, it is reassuring that the majority of individuals are aware of restrictions imposed upon the female interventional cardiologist in the cardiac catheterisation laboratory. WIN have previously published a consensus document outlining the risks associated with radiation exposure during pregnancy, concluding that no data are currently available that adequately demonstrate the actual radiation exposure to the foetus in women working in the cardiac catheterisation laboratory, but that the reported radiation exposure associated with a risk to the child is nevertheless significantly higher than the current recommended limits for radiation workers.29 However, despite the lack of data, careful monitoring of individual risk during pregnancy and strict adherence to radiation safety protocols is warranted and should be part of guidelines. In this survey, 20.2% of females were allowed to continue to work in the cardiac catheterisation laboratory; however, this is entirely dependent upon the country of work, as there are varying radiation restrictions. For example, in Italy, the law requires the pregnant female to communicate her pregnancy with the director of the hospital and it is absolutely forbidden to enter an exposed area. Radiation limits in other European countries included in this survey are generally <1 mSv.
Limitations
The major potential limitation of our study is that of sampling bias, due to the voluntary nature of the survey. In fact it was up to the radiation workers to choose to respond or not, and consequently the sample may not be generally reflective of the interventional community. Indeed, the high proportion of female respondents in this survey may be a consequence of this being a WIN initiative and an increased likelihood therefore of female participation. A further limitation of our study is the sample size and the lack of an age-matched control group, not working within the field of interventional cardiology. Other confounding factors contributing to the occurrence of orthopaedic conditions and even cancer are not taken into account in this study. In addition, the questions are reliant upon self-reporting of illness without documentation or confirmation of this and the survey did not allow for multiple responses to questions, forcing the respondent to choose one answer, which is not so clear-cut in the real world and may have resulted in an underestimation of problems such as orthopaedic issues. However, there was a box stating “other”, which allowed for free text and therefore more than one problem could be included.
Conclusions
Interventional cardiologists and cardiac catheterisation laboratory workers have the highest radiation exposure among healthcare professionals. Training and monitoring radiological protection is therefore of utmost importance. Our survey suggests that orthopaedic problems are frequent among workers in interventional cardiology. Finally, monitoring by dedicated registries of workers in interventional cardiology are necessary to detect long-term effects of radiation such as cancer.
Conflict of interest statement
A.S. Petronio is a clinical proctor for Medtronic. The other authors have no conflicts of interest to disclose in relation to this manuscript.
