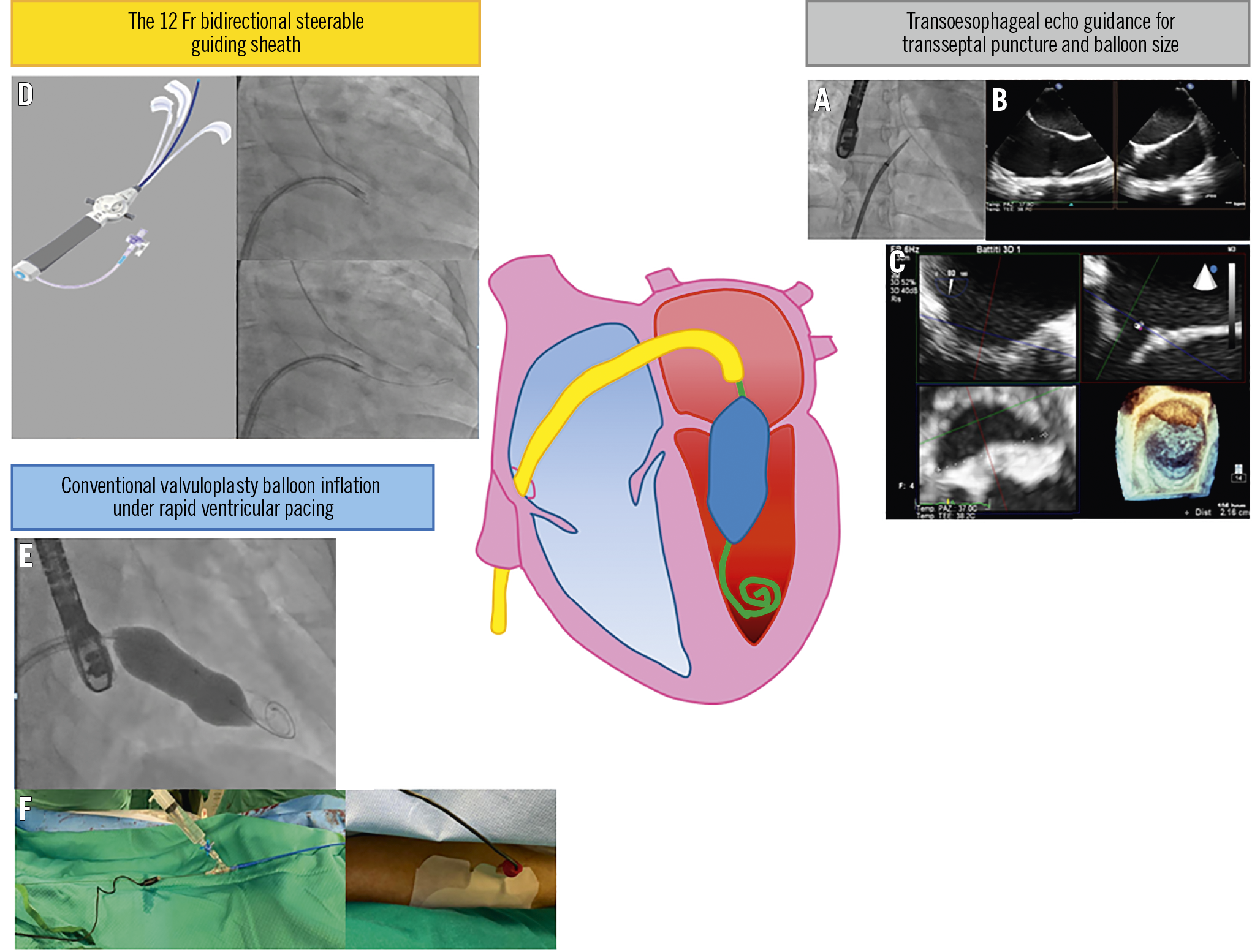
Figure 1. Strengths of the novel technique for percutaneous mitral valvuloplasty.
The Inoue technique is the most widely practised technique for percutaneous mitral valvuloplasty (PMV), but its equipment and technical steps differ from other contemporary structural heart interventions. This has made PMV cumbersome in countries with a low prevalence of rheumatic disease. We developed a novel technique based on the original combination of tools commonly used for other structural heart interventions.
The procedure is performed using the femoral vein to perform the PMV and the radial artery for the introduction of a pigtail catheter in the left ventricle (LV) to monitor the procedure. The key procedure steps (Figure 1) are as follows.
– Transseptal puncture under transoesophageal echocardiographic (TEE) guidance (Figure 1A, Figure 1B).
– The 12 Fr bidirectional steerable guiding sheath (GS) facilitates the crossing through the stenotic orifice allowing the deflection of its tip to face towards the mitral valve (MV) orifice (Figure 1D, Moving image 1).
– Conventional valvuloplasty balloon inflation under rapid pacing to stabilise the balloon position (Figure 1E, Moving image 2).
– Rapid pacing performed non-invasively by directly stimulating the LV (by clipping a crocodile electrode of an external pacemaker onto the guidewire and the other crocodile electrode onto a percutaneous pacing pad located on the patient’s leg1) (Figure 1F).
– Choose the first balloon size according to the virtual intercommissural distance of the MV as measured by three-dimensional echocardiography (instead of height-based balloon reference) to limit severe mitral regurgitation risk (Figure 1C).
– Evaluation of the result by both TEE and invasive gradient control (easily taken by recording left atrial pressure from the GS and LV pressure from the pigtail catheter).
– Possible repeat balloon inflations with the same balloon or with stepwise increased balloon sizes without valve re-crossing in unsuccessful results.
A consecutive series of seven patients with symptomatic mitral valve stenosis has been treated with this novel technique in our centre. In three cases a second (2 mm diameter increase) balloon was needed. The PMV was successful in all patients.
In conclusion, we propose a novel technique with the following strengths: easy antegrade MV crossing, continuous access to the LV over the wire, easy measurement of invasive transmitral pressure gradient monitoring to guide the procedure.
Conflict of interest statement
F. Burzotta discloses having been involved in advisory board meetings or having received speaker’s fees from Abbott, Abiomed, Medtronic and Biotronik. C. Trani discloses having been involved in advisory board meetings or having received speaker’s fees from Abbott, Abiomed, Medtronic and Biotronik. C. Aurigemma has been involved in advisory board activities or has received speaker’s fees from Abbott, Abiomed, Medtronic and Biotronik. E. Romagnoli has been involved in advisory board activities or has received speaker’s fees from Abbott, Abiomed, and Medtronic.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Pigtail crosses the stenotic orifice. The pigtail crossing is facilitated by deflection of the bidirectional steerable guiding sheath.
Moving image 2. Conventional valvuloplasty balloon inflation under rapid ventricular pacing, performed using non-invasive left ventricular stimulation by the stiff guidewire.