“Europe is only a geographical expression”. Metternich said the same about Italy after the defeat of Napoleon and the Vienna Congress closed the chapter on the Italian Republics (later Kingdoms). It was certainly true during two devastating world wars caused by hatred and rivalry among the European powers, but nowadays the biggest conflicts are the clashes between fans during the football cups. With a European Union created more than 50 years ago and a single currency (at least for most countries) for a decade, we may dismiss the statement as ungenerous, but we all know deep in our heart that there is some truth in it. The European Community is certainly a reality for industrialists and bankers allowed to play on a bigger market, but most European citizens feel minimally affected by the European institutions or, worse, Europe is presented by national politicians as the scapegoat for their mistakes and prodigality, forcing strict economic plans impinging on the quality life of ordinary citizens in the weakest partner countries.
What about professionals?
Doctors (and interventional cardiologists in particular) have limited time for culture, possibly less for local and national politics, almost certainly no time for European politics. I prefer not to embarrass colleagues by asking the name of the President of the European Commission (yes, Barroso, Portuguese) or the countries holding the rotating presidency this year (when I am writing this article Hungary, Poland after July1st). Still, the principle of free movement of doctors within the European Community, and the consequent homogenisation of the curriculum of medical schools and postgraduate training, has greatly affected the profession. The principle of subsidiarity means most decisions in health matters are taken by the national or regional governments, but EU citizens are entitled to emergency treatment anywhere in Europe and a push from the EU authorities toward standardisation of at least this aspect of medical assistance would be desirable. Medical Societies lobby in Brussels to obtain resources for research, and we are vaguely aware that drugs must receive approval from a unified European body (The European Medicine Agency, the EMEA) before filing for approval and reimbursement in individual European countries. We discussed in one of these President’s pages a potential greater role of Europe on regulation of devices, similar to the role played by the FDA in the United States1,2. We concluded that there are risks in adding a new layer of bureaucracy because after the CE mark there is also a national clearance process for reimbursement, but we also agreed that there is certainly space for improvement –especially in the critical aspect of post-marketing surveillance– where all European countries play a role as separate entities, with no communication between them3,4.
The role of Europe in medicine
Fortunately Europe plays a much bigger role in medicine than its still weak institutions. The system is different in each country, from the 100% National Health Service (NHS) in Britain and the Scandinavian countries to the various mix of public and private enterprises in Central and Southern Europe, but the principle that every citizen is entitled to free medical assistance is widely applied, a big difference when compared with the reality in the rest of the world, USA included. Social medicine is one of the few legacies of socialism likely to survive the death of this ideology. Irrespective of their political orientation, few doctors will be happy to live in a context where the inprint of their patient’s credit card adds to the delay of primary angioplasty and discriminates against some unlucky individuals unable to afford this “luxury”. The other side of the coin is that you cannot only think in terms of immediate advantage of the individual patient you are treating, but are forced by limited resources to find a balance between quality and cost of service, accepting targets and priorities. In interventional cardiology, the European compassionate approach means liberal use of PCI in ACS, but attention to avoid angioplasty of prognostically irrelevant lesions, large use of transcatheter aortic valves in poor surgical candidates or inoperable patients without extending the application to moribund patients with little to gain in terms of quantity and quality of added life. Europe is a mixture of good and bad for interventional cardiology, with an environment hostile to nurturing companies investing in innovative practice, but still the fatherland of many inventors of devices in interventional cardiology, often forced to move abroad, like Andreas Gruentzig. An exception, but mainly backed by US venture capital, is Israel, proudly becoming the new medical Silicon Valley of Europe. The rest of Europe still misses academic institutions engaged in the practical development of new techniques with number of publications and amount of grants perceived as the only matrix for selection, without much discrimination based on the clinical relevance of the research carried out. Europe misses competent financial analysts and entrepreneurs joining invention and capital, and does not have the resources poured in by the NIH, the NHLBI as well as large academic institutions in the US, now copied by forward looking governments in the Far East.
Evolution of our global presence
It is a common saying that the European century was the 19th, the American century the 20th while the 21st is going to be the Asian century. In 2050, Europe is expected to host less than 5% of the world population and we may expect a demographic shrinkage that does not lead to economic or intellectual growth. The bindings created by common languages and two-way emigration make Europe still a logical choice when it comes to medical education for young professionals in many countries around the world: we must treasure these potential energies and stop applying super-protective policies preventing them not only from practicing, but also from training in Europe. Fortunately, the European medical societies extend far beyond old Europe, and take advantage of the ruthless policy of the European colonial powers to carve empires in Africa, South America, Asia and Oceania. Geographically, Europe is a small appendix of Asia, but when you look at the map of the countries who are members of the European Society of Cardiology (Figure 1), we can call the Mediterranean Sea again the Mare Nostrum like the old Romans did; large countries in Central Asia with historical binds with undoubtedly European nations such as Turkey and the Russian Federation, who are also already part of the ESC or are candidates for membership in the ESC. With 54 member countries and many other affiliated nations the ESC and our Association must look beyond local or provincial interests and reflect this global composition. Despite punitive legislation recently implemented in some European countries to prevent the pharmaceutical and device industry from sponsoring attendance to medical congresses –along with the schizophrenic attitude of governments which police continuous medical education without providing resources– the attendance of both the ESC congress and EuroPCR is still growing every year. Most of this increase comes from outside Europe, with countries like Japan contributing more abstracts than most of the largest European countries. This expansion should be reflected in a more international composition of the Programme Committee of the Congress.
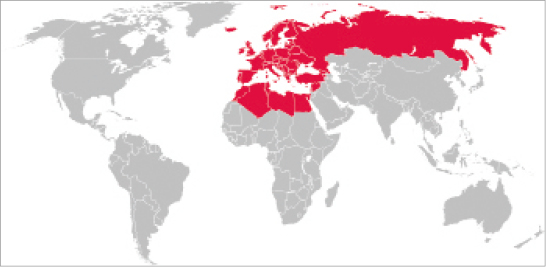
Figure 1. Map showing in red the 54 Member countries of the European Society of Cardiology.
I am writing this in a plane heading to New York, looking forward to an endless queue to leave fingerprints and take photographs like a criminal. Hopefully, Europe will maintain its more welcoming attitude towards foreign visitors which also helps boosting attendance. Successful initiatives of the ESC led to sessions in the main cardiology congresses of China, Brazil, Mexico, Argentina and many other countries, thus supporting the image of Europe as a primary source of education in cardiology and promoting the ESC Guidelines and journals5. Our young Association is involved in these initiatives, but may also take advantage from the entrepreneurial spirit of Professor Jean Marco, Mr. Marc Doncieux and PCR, successful in establishing a well attended AsiaPCR course in Singapore6, and now venturing in a similar initiative in the Gulf area7. The truly international authorship and readership of EuroIntervention is another good example of European leadership in education and research, with over 35% of submissions now coming from non-EU countries.
Maybe not entirely to our merit, but following the footsteps of the Spanish conquistadores and the Czarist army, the weight of Europe in interventional cardiology has grown far beyond its physical dimension and population. Maintaining and expanding this leadership is a challenge for the future officers of EAPCI. I am leaving my Presidency full of confidence that the big internationally recognised champions you have elected after me will further develop this cosmopolitan spirit and foster the European tradition of openness to innovation, compassionate clinical practice, excellence in education and research.
References