My early experience with clinical trials began in the 1960’s, the dawn of cardiac surgery. The FDA was not involved with devices, the concept of informed consent did not exist and the environment was less litigious than at present. It was pretty easy to embark upon a clinical study under those circumstances. Our first patient (Figure 1), had two previous commissurotomies for calcific mitral stenosis.
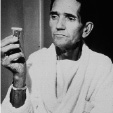
Figure 1. The first successful mitral valve replacement patient and his heart valve.
He is holding a hand-made acrylic valve by Lowell Edwards. Edwards made three of these; one was in the patient, the other in his hand, and the third at the Smithsonian Museum in Washington, D.C. He lived another ten years after surgery (Figure 2) and died of an accident at home while cleaning his roof.

Figure 2. The first patient lived almost 10 years after operation with perfect quality of life.
He had no complications. We did the second patient the following month in 1960, a young lady from Hong Kong with severe rheumatic valvular heart disease (Figure 3).

Figure 3. The second patient also had an uneventful recovery.
This time the valve was of stainless steel. Our first double valve and triple valve replacements (Figure 4), were done in 1963. We devised our own consent form for these early patients.

Figure 4. First double valve replacement patient shaking hands with the first triple valve replacement patient.
What is the patient’s perspective?
The first element I believe is that of trust. If you are setting up a clinical trial you have to establish a relationship with the patient based upon trust. They have to trust the provider, they have to feel that the hospital they are in is a great place and have no reservations. They also have to feel that the device that is going to be implanted has really been carefully assessed and is ready for human implantation –and they have to trust you about that because they cannot investigate it themselves. Also, the patient has to feel that after they have this device they are not going to be abandoned –that you will be there to provide ongoing care for them so if they do have an adverse result, or were randomized to a treatment that was not effective, they could get back into the mix and get appropriate treatment. They also have to understand why there is not a standard treatment for their condition –why a clinical trial is necessary. It has to be in a language that they understand, and yes, it is possible to do that. Patients are also interested in what is the cost to be in the study, what are the economic benefits–: Will there be complications that they might have to pay for, and can they afford these? The patient needs to be thoroughly educated about their disease so that they understand why we are proposing this particualr clinical trial to them in the first place. One caveat, if there is a history of litigious activities on the part of a patient being proposed for the study, I would be very cautious about including them.
A recent review of a Harris Poll1 concerning clinical trials reported that 83% of adults believe that these trials are essential to the advancement of medicine, and 61% of adults polled were confident that participation in clinical trials contributes to medical knowledge and will help other people in the future as well as themselves. However, it was interesting that only 13 to 32% of adults were confident that clinical trial enrollees would actually receive good medical care: that they would, in fact, be treated as patients and not as guinea pigs; that they would be honestly informed of the risks involved; that they are not being recruited for physician or hospital financial gain and that finally they would not suffer more pain or side effects than standard treatment. So there is a lot of suspicion out there on the part of patients that impinges upon their enrollment in a clinical trial, that is why it is so important to establish their trust and go through the steps previously mentioned.
What are the ways to increase patient recruitment? We must have good communication with the patients and their families –as well as other health care professionals that they are dealing with about the importance of these trials. It is not just for their treatment we must insist, but for the advancement of medicine itself. If it is put to them in this way many patients will take an idealistic view of the procedure. In order to improve communications with patients, we have to be able to simplify the information, we have to provide information in different languages or use an interpreter, and we have to have appropriate discussions to make sure patients understand complex trial enrollment forms2. Another important element is to acknowledge patient’s concerns and address them one by one. We have to explain that the goal of the study is to determine if this new therapy is better or worse, and which patients might do better –they have to be in on the deal here. We have to explain that while few treatment protocols include a placebo arm, if the trial does involve a placebo it is because there is really no standard treatment. If there is a standard treatment, then that has to be included in the placebo arm. We have to use social workers to assist patients with time/transportation issues, especially if they are elderly. Also if they have any problems concerning health insurance we should have the staff assist them in defining what role this may play in the clinical study. Another way to increase patient recruitment is to show side benefits of enrolling in the study, for example the patient may be evaluated more frequently than they would by their family physician and this intense follow-up would be to the patient’s benefit. Also they must be reassured that they may have the opportunity to receive the study device after randomization if they are randomized to a less effective treatment arm.
A good enrollment method in clinical trials is to include patient “consultants” early in the trial design; in other words, try the language and approach out with a few intelligent patients –get their feedback– and use this information to make the study more acceptable to subsequent patients. You have to design study protocols that are in harmony with the patient’s goals, for example: Are you using any tests to identify that they are really likely to benefit? Is the protocol a reasonable choice? Is there a potential to cure or improve survival? Will it limit future treatment options? Does it have the potential to improve quality of life and performance3? Now the limitation of treatment options is a very important consideration when randomizing surgical options because if, at the time of an operation, you give some patients a mitral valve repair plus a Maze operation, and the control group a mitral valve repair without a Maze operation, then following both groups up for a long time... well you have lost the opportunity to do the Maze, because the chest is already closed and it is after surgery. So a randomization that leads to a missed opportunity has to be looked at very carefully.
I mentioned randomization and there are some real problems with randomization in regards to ethics, acceptability and feasibility4. I have had some experience with randomized surgical trials when coronary bypass became available at the Oregon Health Sciences University. We randomized medical treatment and bypass surgery and what happened was the patients simply bypassed the hospital. They just would not accept the randomized study, feeling that they were being denied effective therapy –that it was not a fair deal. Therefore, we have to approach these randomized studies very carefully and give the patient a break on both arms of the study and then they will find it acceptable under these circumstances.
This is a picture of our early clinical trial (Figure 5), representing what happens when it is successful.

Figure 5. Dr. Starr and valve patients celebrate 30 years of heart valve replacement.
During our 30th anniversary there was a stadium filled with valve patients, every patient had 1, 2 or more artificial valves. It was a great experience.