Abstract
The spectrum of potentially successful treatment options for inoperable valvular disease is limited. Aortic valvuloplasty may offer temporary improvement in symptoms and some survival benefit in select non-surgical patients with aortic stenosis, but it does not improve long-term outcome. Mitral valve incompetence often responds well to surgical repair, though patients with significantly reduced left ventricular function have worsened outcomes. The design of a percutaneous implantable prosthetic heart valve is a promising alternative to valvuloplasty. Although not yet an established interventional method, Percutaneous Aortic Valve Replacement (PAVR) will likely take a position among the innovative catheter-based techniques currently in development. The appropriate clinical scenario for Percutaneous Mitral Valve Intervention (PMVI), however, may be significantly narrower. As with many other minimally invasive operations or procedures, the ethical considerations of a novel approach must be considered.
Introduction
In 1992, Andersen et al described the first percutaneously delivered bioprosthetic stent valve in pigs1,2. Bonhoeffer et al performed the first human implantation of a similar valve eight years later3. Since the year 2000, a number of novel percutaneous approaches have been developed for Aortic valve Stenosis (AS), aortic valve insufficiency, Mitral valve Regurgitation (MR), and stenotic vessels in congenital heart disease.
In certain patient populations, aortic valve surgery for aortic stenosis remains a high-risk endeavour. Specifically, those patients with severe left ventricular dysfunction, low gradient/low output states, cardiogenic shock, and/or significant comorbidities, such as diabetes, chronic kidney disease, prior cardiac surgery, chronic pulmonary disease, or extracardiac arteriopathy are at the greatest risk4. All are presented with few choices aside from medical therapy or Balloon Aortic Valvuloplasty (BAV)5-8. Vaquette and colleagues reported a 30-day operative mortality of 12% for patients with NYHA class III or IV heart failure undergoing aortic valve replacement (mean valve area 0.6 cm2)9. Nishimura and colleagues demonstrated decreased survival for those patients undergoing aortic valvuloplasty with a low cardiac index, low aortic valve gradient and significant aortic stenosis compared with those patients who had a higher aortic valve gradient with aortic stenosis but similarly low cardiac index. Patients with surgically prohibitive comorbidities and severe aortic stenosis requiring major non-cardiac surgery may also benefit from valvuloplasty. In all of these sub-select populations, BAV remains a mainstay of treatment. However, the procedure is a non-durable treatment with most patients requiring repeat BAV within eighteen months. Percutaneous aortic valve replacement in these groups would represent a more definitive option especially considering that many patients present with different degrees of aortic insufficiency excluding them from any life-saving therapy. Currently there are three companies with clinically advanced percutaneous aortic valves: 1) Percutaneous Valve Technologies/Edwards Lifesciences, with an equine pericardium valve on stainless steel stent; 2) Core Valve, with a tissue valve on nitinol stent 3) Palmaz/Bailey with a nitinol membrane on nitinol stent. The valves are deployed either through a retrograde aortic approach or an antegrade trans-septal approach with sheaths as low as 20 French10.
Mitral valve repair remains the treatment of choice for mitral regurgitation. Enriquez-Sarano recently demonstrated that patients with an effective regurgitant orifice of greater than or equal to 40 mm2 had an increased risk of death from any cause and cardiac death11. However, the repair of mitral regurgitation in patients with severely decreased ejection fraction remains controversial. In this cohort, a less invasive approach to repair would be ideal. Alfieri described the edge-to-edge technique for mitral regurgitation in 1991, which anchors one mitral leaflet against the other using a simple stitch. In one series 89% of patients were free from re-operation at four years12. This led to the development of a percutaneously deployed clip device that consists of a metal alloy covered with biocompatible polyester fabric to enhance endothelial growth. The clip is positioned perpendicular to the mitral valve leaflets to grasp the free edges at the site of regurgitation13. Another percutaneous approach to mitral regurgitation involves the reduction of the mitral annulus size or annuloplasty, a common part of open mitral valve repair. To date, proof-of-concept has been tested in animals and human implantation will likely begin in 2006.
Aortic valvular stenosis: the “inoperable” patient
As clinicians, we are often faced with the “inoperable” aortic valvular heart disease patient and the options for treatment are limited. Therapeutic decisions are typically driven by symptomatology as well as haemodynamic data. With the onset of symptoms, however, life expectancy is less than 2-3 years. When presented with symptomatic severe aortic stenosis in a high-risk patient, consideration for BAV is reasonable14. Many of these patients have low contractile reserve, which predicts high operative mortality and single or repeat BAV may be a palliative procedure.
The question then becomes how one can proceed prospectively in the “inoperable” patient. A retrospective analysis of 212 consecutive non-surgical patients with severe calcific aortic stenosis who had BAV performed by Sharma’s group, demonstrated a median survival rate of 35 months with an improvement in peak transaortic gradient, aortic valve area and symptoms for 18±3 months. During the follow-up period of 32±18 months, 24% of the patients had a second BAV and 9% of patients required a third BAV, with alleviation of symptoms for 15±4, and 10±3 months, respectively (Figure 1).
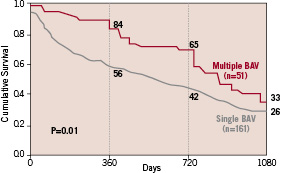
Figure 1. Survival curves of patients who had single versus multiple BAV.15
A fourth valvuloplasty was not recommended as this conferred a high incidence of aortic insufficiency and morbidity. Of note, patients requiring repeat BAV had higher survival rates than those who had a single BAV15. In fact, for many patients with repeat BAV, the quality and extent of life has been prolonged for 4-5 years. The decision to proceed with valvuloplasty, however, is determined by very strict criteria.
The introduction of the European System for Cardiac Operative Risk Evaluation (EuroSCORE) in 1999 was intended to be a predictor of operative risk from cardiac surgery4. The bedside use of this system simply calculates a percent-predicted mortality by assigning weights to particular variables, but this may overestimate or underestimate the mortality risk in certain surgical patient populations. Recently, Roques et al proposed using the logistical regression equation (available at http://www.euroscore.org), as the formula was initially designed, to more accurately predict surgical risk16. For clinicians, this has become a standard by which operative mortality can be determined and the basis of referral patterns for BAV in those deemed poor surgical candidates.
Opportunities for percutaneous aortic valve replacement
Calcific aortic stenosis is the most common valvular disease observed in Western countries. In the next 5 years, aortic valve replacement is expected to increase by 5% per year giving a total number of 180,000 cases worldwide. Of these, nearly 10% are considered high risk and approximately 15%, or about 20,000 cases, are declined by the patient or the physician10. It is this significant cohort of patients for which Percutaneous Aortic Valve Replacement (PAVR) may become the treatment of choice.
The design of a percutaneous implantable Prosthetic Heart Valve (PHV) is a promising alternative to valvuloplasty. Currently available prosthetic valves provide a valve area of > 1.5 cm2, which is a marked improvement over the maximal 1.1 cm2 provided by valvuloplasty alone17. Early pig studies demonstrated important haemodynamic improvements with the use of a bioprosthetic valve implanted within a wire-based stent at assorted aortic sites via catheter technique1. This led to other large animal studies and finally to human subjects.
The initial studies of PHV replacement in children with congenital heart disease were performed in a stenotic right ventricle to pulmonary artery conduit and reported in the year 20002,3. Subsequent reports by Boudjemline and Bonhoeffer described percutaneous implantation of the aortic valve in animal studies, and similar work by Lutter et al, highlighted the problems with subcoronary positioning and potential risk of damage to the mitral valve in animal models18,19. Ultimately, in late 2002, Cribier, et al performed the first PAVR in a 57-year-old man with severe calcific aortic stenosis (bicuspid valve), cardiogenic shock, and peripheral vascular disease in whom valvuloplasty was performed without benefit20. A dobutamine stress echocardiogram revealed no myocardial contractility reserve conferring significant operative risk. Using an antegrade approach, the PHV was placed during cardiac standstill (pacemaker driven) using the native valvular calcification as a landmark. A supra-aortic angiogram confirmed patent coronary ostia. Haemodynamics and placement were confirmed both angiographically and by transoesophageal echocardiogram immediately post-procedure and at day 7 and every 2 weeks following. Clinically, the patient had remarkable improvement in signs and symptoms of heart failure, but ultimately expired from septicaemia-associated complications secondary to an ischaemic limb and amputation surgery. Subsequent procedures on 20 patients performed in compassionate cases (i.e., imminent death) were reported in 2004, demonstrating a viable approach to severe calcific aortic stenosis without coronary occlusion or PHV dislodgement, all resulting in notable clinical and haemodynamic improvement21. Although 12 patients suffered from non-cardiac deaths, eight are still surviving.
There have been two approaches for BAV that have also been followed for PAVR: retrograde via the femoral artery and antegrade with transseptal puncture. At the present time, however, the retrograde approach is the predominant choice since it prevents damage of the papillary muscles, chordae tendinae and subsequent mitral regurgitation recently reported with the antegrade approach22. The antegrade/transseptal technique can be used only in the specific circumstances of severe peripheral vascular disease. As with standard percutaneous procedures, local anaesthesia and mild sedation are used for patient comfort, as are standard arterial closure devices. The native valve is pre-dilated with a 23 mm balloon. Rapid pacing of the right ventricle at 200-220 beats per minute during balloon inflation within the aortic position is used to avoid balloon instability and for transient blockage of blood flow21.
In 2004, Cribier and colleagues reported the results of PHV implantation by antegrade/transseptal approach in 6 patients with New York Heart Association (NYHA) Class IV heart failure23. In each patient, aspirin (160 mg) and clopidogrel (300 mg) were administered the day prior to the procedure and 5,000 IU of heparin were administered during the catheterisation. In 5 of the 6 patients, the PHV was successfully implanted in the subcoronary position (14 mm long stent placed at mid-aortic valve position). Echocardiographic follow-up studies revealed an increase in aortic valve area from 0.49±0.08 cm2 to 1.66±0.13 cm2 (p < 0.04) and a decrease in the transaortic gradient from 38±11 mm Hg to 5.6±3.4 mm Hg. In each of the 5 patients with successful aortic PHV implantation, a dramatic clinical improvement in signs of heart failure was described. Paravalvular aortic regurgitation was noted in all 5 patients and was attributed to imperfect approximation of the stent frame to the heavily calcified native aortic valve. As mentioned, however, with the antegrade/transseptal approach, there is recent evidence of complicating mitral regurgitation22.
There have been a total of 80 patients that have had PAVR in 2005, as provided by the manufacturing companies. The follow-up period is quite short, however, and survival ranged from 66% to 78% of those successfully implanted (Figure 2).
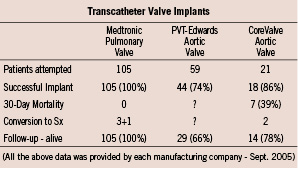
Figure 2.
This is clearly a technology that is evolving, but there are many important issues still to be addressed.
Although not yet an established interventional method, PAVR will likely take a leadership position among the innovative catheter-based techniques currently in development. As with many other minimally invasive operations or procedures, the ethical considerations of a novel approach must be considered24. With the evolution of this technology, we must consider when and to whom such a procedure is recommended. For the cohort of “compassionate cases”, appropriate review by the institutional ethics committee as well as informed consent by the patient and/or the closest relative should be obtained. Prior experience dictates that the mortality may be quite high during the early years of an innovative procedure for a complex cardiac entity, as was the case in the 1950s with intracardiac repair for Tetralogy of Fallot25.
In the next 5 years, as PAVR becomes more mainstream as a reasonable and effective strategy for symptomatic patients with severe aortic stenosis, it will be important to safeguard this technology by restricting it to high volume centres of excellence. The greatest benefits, however, may be realised in patients that are less sick and who would have otherwise been referred for aortic valve replacement surgery.
Mitral valve incompetence: wide scope of valve and natural history complexity
Mitral Regurgitation (MR), may lead to left ventricular dysfunction, right ventricular dysfunction and heart failure. Ischaemic heart disease and myxomatous degeneration make up the majority of cases in the western world. Carpentier first classified MR by the mechanism of abnormal leaflet motion into three groups: those with leaflet perforation or annular dilatation; increased leaflet motion secondary to chordal dysfunction; or restricted leaflet motion due to rheumatic disease or papillary muscle dysfunction26.
Untreated, severe MR is clearly associated with increased morbidity and mortality regardless of the mechanism of valvular dysfunction. In a Mayo clinic cohort study of 773 patients examined by echocardiography after myocardial infarction, 50% were found to have MR, of which 24% had moderate to severe regurgitation (Figure 3)27; many cases had not been noted on clinical examination.
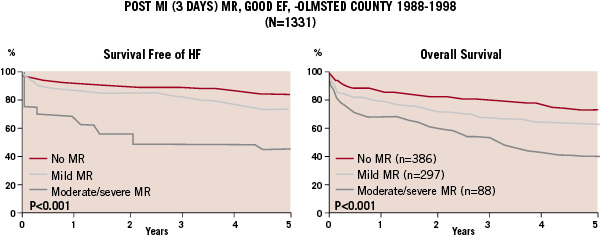
Figure 3. Heart failure and survival with varying degrees of MR.27
Over a five-year follow-up, there was a significant association between severity of MR and development of heart failure or death, after controlling for ejection fraction, Killip class, age, and gender. In patients surviving the first 30 days after myocardial infarction, moderate to severe MR increased the risk of death by 55%, even after adjustment for other comorbidities. Annually, the risk of death in this group was exceedingly high at 10%. In addition, patients with mild MR post-myocardial infarction often progress to more significant MR over time and their risk may increase concomitantly.
Even without implicating cardiac failure in patients with preserved left ventricular function, severe MR is clearly associated with increased morbidity. Enriquez-Sarano et al found that effective regurgitant orifice (ERO) as measured by Doppler echocardiogram strongly predicted both mortality and cardiac events over a five-year period11. Survival in patients with an ERO greater than 40 mm2 at five years was 20% lower than expected. There was a graded increase in risk of death as ERO increased, independent of the mechanism of mitral incompetence, with a risk of cardiac mortality nearly 50% at five years in the group with an ERO greater than 40 mm2. Otherwise, cardiac events, including heart failure and new atrial fibrillation, also increased in proportion to severity of regurgitation.
Surgical risks and benefits
In general terms, surgical intervention is indicated in some asymptomatic patients with evidence of severe MR, such as those with left ventricular dysfunction, pulmonary hypertension, right ventricular dysfunction or atrial fibrillation; and certainly is indicated in the majority of symptomatic patients, unless left ventricular function is significantly affected.
As it relates to the impact of left ventricular function in the surgical results, surgical intervention has been shown to increase event-free survival in patients with severe MR, particularly those with preserved ejection fraction. In one study of patients with a flail mitral leaflet followed over 10 years, multi-variable analysis showed that surgical correction of the mitral valve was associated with a significantly reduced mortality rate regardless of the timing of surgical intervention. Early surgical treatment prior to the development of severe progressive left ventricular dysfunction clearly improved prognosis in this group28. The less encouraging surgical results in patients with MR and significant left ventricular dysfunction bring into consideration the approach with mitral valve repair versus replacement.
Surgical mitral repair has been associated with improved mortality outcomes, reduced operative complications, and better postoperative ejection fraction compared to valve replacement. Overall, in experienced surgical centres, isolated surgical mitral valve mortality is about 2% with repair and about 6% with replacement28. In patients over the age of 60 years, long-term survival also favours repair. Collectively, operative mortality with combined CABG is about 8% vs. 12% in repair and replacement respectively. However, patients with a severely calcified mitral valve and rheumatic disease, or significantly dilated mitral annulus, may not be good candidates for repair. Importantly, a Left Ventricular Ejection Fraction (LVEF)>35% was associated with a significant reduction in 5 year mortality to 18% after mitral valve repair in a study by Talwalkar et al (Figure 4)28.
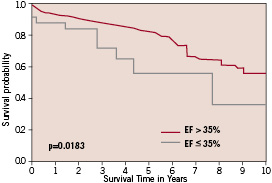
Figure 4. Survival estimates after mitral valve repair with EF above or below 35%.28
Reduced ejection fraction is associated with poorer outcomes in patients undergoing mitral valve repair. In Talwalkar’s retrospective analysis, the group of 36 patients with LVEF ≤ 35% had significantly elevated peri-operative mortality (8% vs. 2%) and a reduced five-year survival (54% versus 82%) compared to those with relatively preserved LVEF. Ischaemic heart disease and NYHA class were associated with significant increases in mortality, particularly in conjunction with low LVEF. In patients with left ventricular dysfunction, which often leads to alterations in the geometry of the mitral valve annulus and significant MR, mitral valve annuloplasty has not been shown to improve long-term outcome. Although short-term symptoms and cardiac functional indices appear to improve with annuloplasty, in this group, Wu et al showed that long-term outcomes do not follow this trend. In her retrospective study, 126 patients undergoing mitral valve annuloplasty for moderate to severe MR did not have any significant difference in long-term mortality, or progression to left ventricular assist device or transplantation, compared to the group who were candidates for surgery but declined29. No significant differences were seen in the subgroup without coronary artery disease when analysed separately. Mitral valve repair in patients with significantly reduced ejection fraction may not provide significant benefit. Combined surgical treatment of ventricular dilatation and mitral regurgitation for patients with impaired left ventricular function may be considered in the future.
The narrow window for percutaneous mitral valve repair
A variety of surgical approaches to mitral valve repair have been described, including mitral annuloplasty, chordal reconstruction, and leaflet repair. An edge-to-edge technique, in which scallops of the anterior and posterior leaflets are approximated, resulting in a double-orifice mitral valve, was described by Alfieri and has more recently been utilised for repair12. Surgical correction is the standard of care for valvular incompetence, and depending on the mechanism of regurgitation and the experience of the surgeon, minimally invasive surgery is sometimes an option. Given the excellent results in surgical repair for MR with preserved ejection fraction, experimental percutaneous treatments will have a high standard against which to compete. On the other hand, the dismal results in patients with significant left ventricular impairment make surgical approaches of any kind a significant risk. Therefore, the window for development of percutaneous Mitral Valve Intervention (PMVI) may be quite narrow.
Evolving PMVI approaches to treatment of MR that limit surgical morbidity while providing the improved outcomes associated with surgical intervention are in very early stages of development. A percutaneous approach involving transseptal puncture was recently developed. In the phase 1 feasibility and safety trial, the Endovascular Valve Edge-to-Edge Repair Study (EVEREST), 27 patients with moderate to severe MR and either symptoms or left ventricular dysfunction underwent percutaneous mitral repair30. Ninety-three percent had degenerative MR and the remainder had ischaemic MR. Eighteen of 24 patients receiving clips (75%) had successful device deployment with resultant decrease in MR to < 2+ on discharge. There were four partial clip detachments and one stroke at > 72 hours that resolved at one month. At thirty days, 85% of patients were free from major adverse events. Thirteen of the 18 retained MR of < 2+ at 6 months, resulting in a modest 54% success rate. This is far less than the current success rate for surgical repair. In addition, the majority of the study group (66%) had NYHA Class II or better heart failure symptoms. Although the group had severe MR by echocardiographic definition, the overall cohort was likely low risk.
Alfieri’s edge-to-edge technique may not be as successful without concomitant annuloplasty. A retrospective study of edge-to-edge mitral repair performed without annuloplasty, as in the current percutaneous approach, found an increased rate of recurrence of significant MR compared to the annuloplasty group31. Outcomes were particularly poor in patients with severe annular calcification and rheumatic lesions. The edge-to-edge technique was also examined in 224 patients with moderate to severe MR primarily as a result of ischaemic cardiomyopathy (64%), as well as myxomatous disease and dilated cardiomyopathy32. About 84% underwent concomitant annuloplasty. The majority of patients also had another procedure (CABG, AVR, or LV reconstruction primarily) simultaneously. Although MR was eliminated in 79% of patients at discharge, the number of patients free of MR quickly fell. This was particularly true of those patients with ischemic MR, where over 20% of those without MR at discharge had 3+ to 4+ MR at 3 months. The edge-to-edge technique appears to lead to poorer outcomes in patients with ischaemic cardiomyopathy.
Based on the above information, other percutaneous devices are under development and have undergone initial testing. Kaye et al tested a mitral annular constraint device positioned in the coronary sinus and great cardiac vein, which reconfigures the mitral annulus into a more favourable shape33. Using a sheep model, the investigators induced at least moderate MR through rapid ventricular pacing. The constraint device was successfully deployed in the coronary sinus of nine animals, and MR was absent in seven of the nine animals after device implantation. Phase 1 human trials will likely begin this year. Numerous other percutaneous devices are under development at various preclinical stages, mainly aimed toward a very small group of patients with relatively preserved left ventricular function, yet, who cannot pursue open surgical repair.
The FDA and predictions from industry
The advent of any new technology always involves a blend of enthusiasm and scepticism. The promise of PAVR has already been demonstrated in select cases20. Expectations have been raised and now we await the rigorous clinical testing that is required for any new device seeking approval by the U.S. Food and Drug Administration.
Although the approval process for percutaneous valve technology has been slower than anticipated, it is still moving forward. The use of the devices in the U.S. is currently relegated to Phase I trials or compassionate use, and fewer than 200 total devices have been placed into humans. This is in comparison to the thousands surgical valve replacements or repairs. With the current safety and durability records of surgery, the market for percutaneous placement is currently limited to those patients deemed too high risk for surgery. This number is not insignificant, in one European prospective survey 30% of symptomatic patients with valvular hear disease were deemed too high risk for surgery34. It is hoped that a large majority of these patients would benefit from percutaneous valve replacement. Industry newsletters estimate that the number of percutaneous valve replacements performed by the year 2010 will be about 12,000. The predictions account for an early adoption of percutaneous valve technology for the pulmonic valve, but that by 2015 the majority of interventions will be PAVR and less than 10% will be PMVI. Indeed, at least 10 companies are currently developing the technology. These rosy predictions assume that this technology can be proven both safe and efficacious or it will be limited to compassionate use only10.
The FDA, industry, and academia are all interested in moving this technology forward in a safe but efficient manner. A position paper published jointly by the Society of Thoracic Surgeons, the American Association for Thoracic Surgery, and the Society of Cardiovascular Angiography and Intervention, with input from the American College of Cardiology, the U.S. Food and Drug Administration, the Centres for Medicare and Medicaid Services, and industry representatives, addressed the most critical several questions and provides the framework that is necessary for the approval of these devices35.
General guidelines for testing new medical technologies begin with a feasibility study in a small number of patients to assess safety and design issues. This is then followed by a larger pivotal trial (Phase II) to assess safety and efficacy. The recently published EVEREST I trial provided 6 month Phase I data on the edge to edge mitral valve repair system by Evalve Inc30. The safety data was reassuring and allowed the progression to Phase II pivotal trials. PAVR and PMVI techniques are still in phase I, and mainly limited to patients that are not operative candidates. Edwards Lifesciences resumed its Phase I trial of PAVR in December after a 6 month pause while they improved the delivery mechanism. Among other refinements, the retrograde approach is now being used exclusively. Several important issues arise as the safety trials conclude and the Phase II trials begin. The FDA wants randomised, controlled trials, but the control arm has to be chosen carefully: optimal medical therapy or surgery. Endpoint selection is also important. For MR the endpoint should include reduction of MR to at least 1+ and for aortic stenosis the endpoints should include haemodynamic improvements and clinical events10. The FDA requires follow-up times of at least 2 years.
Conclusion
PAVR and PMVI are a long way from replacing traditional surgical aortic and mitral valve interventions, but it is taking its first baby steps. It is possible to imagine a not-so-distant future when severe aortic stenosis is treated with PAVR.
